|
|

-
-
I) The Ancient East
According to Herodotus the Babylonians had no physicians; the patient was brought out in the market place and all passers-by had to confer with him "to discover whether they have themselves been afflicted with the
same disease or have seen others so afflicted and advise him to have recourse to the same treatment as that by which they escaped a similar disease, or as they have known to cure others."
But the code of Hammurabi with its rewards and penalties for physicians, gives a glimpse of an already more highly organized system at a period earlier than 2000 BC - long before Herodotus. The Code enacts that for a successful operation
which saves the eye of the patient the fee be ten shekels of silver in the case of a "gentleman," but only five shekels and two shekels in the case of a poor man and owned slave respectively. For an unsuccessful operation on a freeman
causing death or the loss of the eye, the surgeon shall have his hands cut off; in the case of a slave the penalty was to replace him by another.
Babylonian medicine was probably in the hands of the priests of the healing divinity Ea and his son Marduk, whilst surgery, as almost everywhere else in early medicine, was in the hands of a special class of skilled hand-workers. The
etymological derivation of surgery is significant for ceironrgia, means handicraft. The priestly, non-operative practice was not regulated by law; but that the work of the surgeons was not
altogether despised is shown by the very liberal scale of fees, for five shekels was equivalent to the yearly rent of a good type of house and represented 150 times the daily wage of a workman (1/30 shekel). The medicine of the priests was
a mixture of superstition and ignorance; treatment consisted of incantations and also the administration of foul remedies - probably to disgust the demons causing the disease. It would appear that the practice of the surgeons was supervised
by the priests. but it is by no means clear what their work was. It is quite possible that the greater part of the Babylonian surgery consisted of couching cataract. On the other hand, the eye operation spoken of may merely have been
incision of an abscess of the lacrimal sac. The whole evidence turns on the significance of an obscure work in the code, naqabtu.
The earliest records of Egyptian medicine date back to a period not much later than the Code of Hammurabi, the Edwin Smith papyrus to c. 1600 B.C., the Brugsch papyrus to c. 1300 B.C. and the Ebers papyrus to c.1550B.C. A
remarkably advanced state of ophthalmology can be inferred from the Ebers papyrus in which a section is devoted to eye disease, treatment rather than clinical descriptions being given. Incantations, foul applications and all the other
manifestations of superstitious ignorance abound, but there is evidence of an advance that must have involved centuries of empirical practice and observation. The most significant development is the recognition of a number of distinct
diseases. According to Ebers the Egyptians knew such conditions as blepharitis, chalazion, ectropion, entropion, trichiasis, granulations, chemosis, pinguecula, pterygium, leucoma, staphyloma, iritis, cataract, hyphaema, inflammation, ophthalmoplegia and dacryocystitis. The attempt at differential treatment implies a degree of differential diagnosis; nevertheless it was still the medicine of the temple that they practised. Indeed the Ebers papyrus is probably the work of
priests, thought it is not, as was once thought, a part of the lost six medical books of Hermes containing the divine knowledge of healing as set down by the Egyptian priests.
There is no evidence that Egyptian surgery had made any marked advance; the only surgical procedure mentioned in the Ebers papyrus is epilation, a practice that must have been widely spread judging from the frequency with
which epilation forceps have been found in relics of the New Empire.
Later development in Egypt brought but little advance, though there is much evidence that Egyptian ophthalmology was held in high esteem in ancient world. Herodotus relates that Cyrus of Persia sent to Amazis, the king of
Egypt, for a physician to cure him of his eye trouble. The decline of Egyptian civilization brought with it that type of specialization which is based not on expert knowledge of a detailed field, but on ignorance of every other subject.
Both the prophet Jeremiah and Herodotus found the country full of physicians and Herodotus remarks that "one treats only the diseases of eye, another those of the head, the teeth, the abdomen, or of the internal organs."
Nowhere in the Ancient East was medicine ever freed from the shackles of supernatural belief. Observation was coloured by preconceived notions of the demoniacal origin of disease. Here and there a glimpse of a modern procedure
is seen, based on methods and premises different from ours. In Hindu medicine there is a suggestion, in the writings of Suçruta, of the earliest record of surgical treatment of cataract by couching. In Hebrew writings there is a textually
obscure reference to improvement of a woman's appearance by having a golden eye (in the place of a missing one), an interesting and significant remark in the light of later history, for prostheses made of gold were the first to be used and
were not introduced until the 16th century at the time of Ambroise Parè. Early Greek medicine differed in no essentials from that of the rest of the ancient world. There was the same priestcraft, the same temple worship and supernatural
cures. Nor were these temples as holy as they seemed. It was only with the rise of the Asclepiadaæ, a group claiming descent from the God Aesculapius, but dissociating themselves from the priests of the temples, that Greek medicine began.
One of these Asclepiads, Hippocrates the Second, also known as Hippocrates the Great, or simply as Hippocrates, born on the island of Cos, finally liberated medicine from the thrall of the supernatural. His method is the method of modern
medicine; the study of disease as an objective natural phenomenon. The lasting achievements of the Greeks are commemorated in the term physician derived from fusiz, natura. Hence forth the
physician was essentially no longer a priest but a naturalist.
II) The Greek Period
Ophthalmology benefited at the hands of Hippocrates and his immediate followers mainly in a negative way - in discarding the supernatural element rather than in any definite advance in the understanding of ocular disease.
Their notions of the structure and function of the eye had hardly advanced, if at all, beyond that which the much older Egyptian civilization knew, though a a predecessor of Hippocrates, Alcmaeon, is credited with the discovery of the optic
nerve. Their recognition of eye disease was confined to what could be observed and deduced from a knowledge limited to the superficial anatomy of the eye combined with an utter lack of understanding of ocular physiology. It is mainly in its
influence on the further development of ophthalmology rather than in its achievement, that Hippocratic ophthalmology is remarkable, though it is well to recall that their treatment of some forms of conjunctivitis by irritation is still the
basis of the modern treatment of trachoma. When they went astray they were wrong in the same way as the modern world is wrong when mistaken treatment is given on the strength of a wrong pathology; their failures were different in nature
from the failures of those who invoked the aid of the gods or attempted to cast out the devil.
Greek medicine stretches over a period much longer than the medicine of the modern period. From the appearance of Hippocrates to the end of the fruitful period of Rome is well over 800 years. During that time there was a
continual development in which ophthalmology shared. Greek medicine soon became extinguished on its native soil but developed apace, first in Alexandria and then in Rome. Of the great achievements of the Alexandrian period one can only
infer by comparing the end of the purely Greek period with the beginning of the Roman period, the actual records of the Alexandrian school having been lost. The study of the human anatomy began in Alexandria, and the earliest Roman writings
on the anatomy of the eye, thos of Rufus, are a measure of the advance made by the Alexandrian school. After the decline of Alexandria, it was in Rome that the Greek spirit found a home. There medicine was so entirely Greek that the Romans
who practised it felt compelled to adopt Greek names for themselves and their remedies. Of the writings of this period there remain thos of Celsus, Pliny and Galen; reference to other writer whose works are lost are to be found in these and
later books. Galen's strictly ophthalmic writings have been lost.
Of a period later than Galen's there are the works of Aetius of Amida and of Paul of Aegina, giving a full account of the medical and surgical practice towards the end of Byzantine period. In Celsus there are detailed
descriptions of couching for cataract, of operations for ankyloblepharon, dacryocycstitis, and of plastic procedures for trichiasis, lagophthalmos and ectropion. Hypopyon is first mentioned by Galen. Of Galen's contributions to
ophthalmology it is perhaps enough to say that nothing of any value was added to his anatomy of the eye till the beginning of the 17th century; his theory of vision was however a grievous errors. The later writers of the Greek period added
some details to the practice of ophthalmology, but nothing whatever to its theory. The beacon lit by Hippocrates and tended by Alexandria and Rome was slowly sinking in a world plunging deeper and deeper into the mists of the Dark Ages.

Numerous busts have survived of the allegedly blind poet Homer. The earliest portrait type, which is
believed to derive from a Greek original dated c.450BC, does not, however, attempt to render his sightlessness in an explicit manner, but merely shows the poet's eyes closed in deep contemplation. Not until the second century BC did any
artist attempt to portray his blindness. One of the earliest such portraits, of which there are several examples extant, has been justly described as "amongst the most beautiful portrayals of poetic genius". The absence of modelling to the
eyeballs, the heaviness of the raised eyebrows, all focus the viewer's attention unremittingly on the eyes. The air of intense, almost rapt absorption and introspection exquisitely captures the inner world of the blind poet.

Commonplace sufferers from eye complaints were not accorded any such deference. A terracotta from Tarsos of an emaciated man in a pointed cap exhibits "a pervasive air of stupidity, corruption and sordid cunning". The eye
are markedly asymmetrical, one being circular, the other a half closed slit. Though the inspiration for this type may have derived from a comic mask, the mask in turn probably represents an attempt to render trachoma, an infectious eye
disease which was probably very prevalent in the ancient world, as it still is in the Middle East today.

Sudden loss of sight was also depicted with some frequency in Attic red-figure, due to the popularity of the myth of the
blinding of Thamyris. On an Attic hydria dated c.430 the musician, whose eyes are closed, registers his pain and terror by stretching out his arms and letting his lyre slide from his lap. Sculptors, too, attempted the subject. Pausanias
tells us that a statue of Thamyris, "already blind and holding a broken lyre", was dedicated on Mount Helikon, sacred to the Muses. It perhaps served as a warning to over-ambitious bards.
III) The Arabian Period
The fitfully flickering flame of civilization was saved from extinction by the invading hordes of the Eastern conquerors sweeping across the known world under the banner of Allah. As before in the case of Rome, so once again
Greece took its captors captive. By means of translations, first into Syriac and later into Arabic, a knowledge of the older Greek civilization was spread throughout the Mohammadean world. Ophthalmology took a new lease of life, though
progress was severely handicapped by the lack of anatomical studies. Hospitals, departmentalized very much in the modern manner, grew up and ophthalmic departments were always large and important. Many operative procedures known to Galen
and his successors were perfected and some important additions were made. Numerous treatises on diseases of the eye appeared, all drawing their inspiration from the Greek writings. But the centuries of Arabian dominance lacked the eager
questing that characterized Greece. The Arabians perfected old procedures rather than explored new avenues; they revered rather than challenged the authority of tradition. So heavily did the hand of dead ages lie upon them, that though
there is much that is valuable in Arabian ophthalmology, it is incidental rather than the result of a conscious effort. Not infrequently they stumbled on facts and conceptions that could not be harmonized with the traditional knowledge,
but they only cut their new cloth into ill-fitting archaic patterns. They had not learnt the crowing wisdom that fact is greater than dogma. It is characteristic of the period that Ali ben Isa (Jesus Hali), Alcoatin and Ammar ben Ali wrote
text-books that were used for centuries.
Like the Western civilization that followed it, the Arabian period was not a national movement. It was Arabian in language only; the men who made it were of that variety of nationality and religion that were to be found
between Cordova and Bahdad. When decay ultimately overtook the Arabian renaissance, the torch had already been handed on to the rising civilization of Western Europe by means of translations into Latin from the Arabic versions of the Greek
masters. Many mistakes were perpetuated by these translations and retranslations and it needed the European renaissance to direct onward the pure stream of Greek thought.
IV) The Western Middle Ages
Whilst the Arabians nursed and revived a moribund civilization, knowledge did not altogether perish in the western domains of what was once the Roman Empire. Here and there in the monasteries intellectual life flickered, and
some stray sparks would be brought by Jews coming from Mohammedan lands. The beginnings of a systematized intellectual effort is found in the schools of Salerno and Montpellier. In the 11th century Constantinus Africanus, a widely travelled
man and at one time teacher in Salerno, translated Arabic writings into Latin, thus beginning a movement that gathered speed with the years. But ophthalmology in those days of twilight was nevertheless little more than a debased handicraft;
couching for cataract, like cutting for stone, was an operation which everyone was allowed to perform, and was in fact left to itinerant practitioners. The regular practitioners of surgery advised against eye operations and paid but scanty
attention to eye disease in general. The writings of Peter the Spaniard (later Pope John XXI) are a treatise on the hygiene of the eye and contain no reference to surgical treatment. The writings of Master Zacharias, a Salernitan of the
12th century, are of little significance but those of Benevenutus Grassus are of considerable importance in the history of ophthalmology. Little is known of the author, but the book had a great influence in spreading knowledge of eye
disease. The original seems to have been written in Hebrew and there are translations in Latin, Provençal, Old French and Old English. There is little new in the book; it is essentially a good summary of Greek and Arabian teaching. The
importance that medieval ophthalmology attached to it can be gathered from the fact that it is the only ophthalmic incunable. Guy de Chauliac and John Yperman were influenced by Benevenutus' book, Yperman himself contributing to
ophthalmology the conception of contagiosity of ophthalmia.
If the Western Middle Ages produced no memorable oculists, it produced geniuses who in their versatility contributed to ophthalmology. Roger Bacon's ophthalmic achievements include the rediscovery of the crossing of the optic
nerves at the chiasma and the first mention of convex lenses for presbyopia., whilst Leonardo da Vinci either realized or came very near to realizing the principle of the camera obscura as applied to the eye.
V) The Modern Period
If the practice of ophthalmology had hardly advanced during the long centuries that followed Greek medicine at its height in the Rome of Galen, it had little to gain at the Renaissance by looking backward. Further advance in
ophthalmology was made possible by the study of the anatomy of the eye, and by an understanding of the mechanism of vision. This was the work of the 16th and 17th centuries and paved the way for the great pathological and clinical progress
of the 18th century, the century of cataract extraction and the artificial pupil. The first half of the 19th century was a remarkable period of consolidation, and the second half brought the operative treatment of glaucoma, whilst the
ophthalmoscope opened a world undreamt of and raised ophthalmology to the most exact of clinical studies.
It was in Arabian literature that figures illustrating the anatomy of the eye first made their appearance. Arabic manuscripts still exists in which reference is made in the text to figures, themselves missing, though space from
them is provided. The earliest drawing as yet available appears in Hunain ibn Is-hâq's Book of the Ten Treatises on the Eye, recently discovered and edited by Meyerhof (frontispiece).
Through lack of
illustrations it is difficult to get a clear conception of Greek and Roman knowledge of ocular anatomy, for the descriptions are frequently not only scant, but confused through a multitude of names, which may or may not have had the same
meaning.
Pre-Hippocratic anatomy had hardly passed beyond the stage of recognizing a transparent cornea continuous with an opaque sclera, the whole being lined by a layer with a perforation which formed the pupil. These two layers
enclosed a fluid substance. This conception of the anatomy of the eye was not based on detailed observation, but on speculation as to the nature of vision. The fluid in the eye was regarded as the principle of vision and a tube leading from
the eye to the brain, allowing for the free movement of this visual substance, led Alcamaeon to postulate the pÓroz, poros.
This postulated hollow tube is hardly the solid optic nerve of modern anatomy. An advance of these speculations is to be found with Aristotle, who obviously dissected animal eye. (Figure 1). Three layers instead of two are recognized,
though knowledge of the retina hardly went beyond the recognition of its existence.

Figure 1. The structure of eye as
conceived by Hippocrates & Aristotle
Knowledge of the structure of the cavity of the eye was vague. There was no recognition of the anterior chamber; it was held that the three layers of the
eye are intimately apposed to each other. The ocular fluid was considered as of uniform consistency, though some differentiation occurred on exposure to air; the lens, as far as it was clearly recognized, was thus regarded as a post-mortem
manifestation. The hollow tube of Alcamaeon became three in number, one of which entered the skull and joined with a corresponding structure from the other eye. The recognition of the chiasma and of ocular vessels had therefore been
achieved.The Alexandrian school contributed largely to the knowledge of the anatomy of the eye. Herophilus in particular seems to have devoted much attention to the eye; from a reference in Aetius it is clear that he wrote a special
treatise on the subject. As no manuscripts of this period have survived one has to rely on Celsus for information (Figure 2), and Celsus' account is by no means clear for the reason, as Hirschberg puts it, that he did not understand the
subject. There is a clear recognition of the existence of the lens, a drop-like body named Krustalloidez, crystalloides.

Figure 2. The eye as decribed by Celsus
Whilst no anterior chamber is indicated — the second layer is
still contiguous with the first, except in the pupillary area, which is a mere perforation — it is recognized that the retina does not come up to the cornea; it forms a smaller enclosing structure, and comes to surround the ocular
fluid including the lens. This arrangement leaves a large empty space — locus vacuus — between the two outer layers and the smaller retina. As this locus vacuus is also spoken of as containing "humor", a near approach to the
appreciation of the existence of the anterior chamber may have been made. What exactly Celsus knew of the optic nerve is not clear: he does not speak of any hollow canal, nor does he speak of a continuation of the retina into the nerve.
The optic nerve probably appeared to him as a continuation of the fused two outer layers of the eye.
With Rufus a much clearer conception of ocular structure emerges. The conjunctiva is recognized, though of course not distinct from the capsule of Tenon, which indeed was not described till 1806. Under the name of epidermiz, epidermis, it is regarded as a fourth covering layer extending from the junction of the cornea and sclera to the posterior pole. The corneo-scleral junction stefauh, stephane, is regarded as also indicating the site where the retina branches off to line the posterior aspect (no longer the anterior) of the lens. The lens itself is invested with a
lining layer, but whether this is a distinct layer or a decomposition product of the lens (?liquefied cortex) is not clear to Rufus. Of significance is Rufus' conception of the internal structure: as Magnus points out, this approaches
the modern view. Two spaces are recognized, one lying between the cornea and iris, and another behind the lens. The first space, a mere chink, was filled with a fluid very much like water, whilst the second contains a substance like the
white of a raw egg. Four serious defects mar the description by Rufus. He failed to recognize the existence of the posterior chamber, the greater curvature of the cornea as compared with the sclera, and the inequality in the curvature of the
lens surfaces; and his reference to the optic nerve is most scanty. These defects were in a large measure rectified by Galen (Figure 3).

Figure 3. The eye as described by Galen
Just how much the description given by Galen is the result of his own observations or that of predecessors is not known. But Galen's account is of significance not only because it marked an advance, but even more because no
advance was on it till after Vesalius. If pre-Hippocratic anatomy was speculative, and Alexandrian anatomy truly descriptive, anatomy after Galen became a historical exercise on which commentators were busy for well over a thousand
years.
A fairly clear recognition of the ciliary body seems to have been arrived at. The corneo-scleral junction — one name for which, incidentally, was iris, a designation that persisted till well into the 18th century — was also the seat of fusion of the choroid and retina, where in addition a layer lining the anterior surface of the lens also terminated. The posterior chamber was clearly recognized, as was also the fact that it contains the same
fluid as the anterior chamber. The greater curvature of the posterior surface of the lens was likewise recognize; the lens itself was held to fuse with the choroid by which it was kept in position.
It should be noted that whilst
the recognition of the greater curvature of the cornea over the sclera was obviously the result of observation, the recognition of the existence of the posterior chamber was the result of speculation. Galen's writings are not clear on the
subject, and as Magnus points out, he could not possibly find a space between the lens and iris in an eye cut open without the modern methods of preliminary fixation; but his theory of vision which postulated dilatation of the pupil by pneuma, called for a posterior chamber through which the pneuma could diffuse on to the lens.
Speculation also entered into the description of the optic nerve. Whilst Galen recognized its solid structure he had to maintain a central hollow canal, in the sense of Alcmaeon. At the chiasma fusion of the hollow canals
of both nerves took place. That Galen drew on animal dissection is clearly seen from his description of extraocular muscles, of which there are seven — the six of present-day human anatomy with an additional massive ensheathing muscle
which arises from where the optic nerve enters the orbit — obviously the retractor bulbi of comparative anatomy. Furthermore, in describing the lacrimal apparatus he speaks of two glands, one in the upper and one in the lower
lid. Galen recognized another source of tears - glands in the conjunctiva of the lids. The conjunctiva itself he held to be derived from the pericranium.
Arabian anatomy was the anatomy of Galen modified not by the evidence of dissection but by conclusions drawn from speculation. Depression of cataract extensively practised; and as the prevailing view was that a corrupted humour in
front of the lens was displaced in the process, it was necessary to conceive the lens as being situated further back than in Galen's scheme. This view as to the seat of the lens persisted till the beginning of the 17th century.

Figure 4. Illustration from
Vesalius (1514-1565)
With the coming of Vesalius, anatomy turned once more from speculation and commentaries to dispassionate observation. But to ocular anatomy Vesalius contributed nothing (Fig. 4). His teaching is distinctly inferior to that of
Galen and even of Arabian ophthalmology. The recognition of the greater curvature of the cornea over the sclera, and of the posterior surface of the lens over the anterior, is lost. A central position of the lens is once more in
evidence. Even more astounding is Vesalius' acceptance of Galen's retractor bulbi.
Modern anatomy of the eye did not emerge till the physicists had demolished the old conceptions of the nature of vision. It began when it was realized that the lens is not the seat of vision, but part of a refractive system. With
Fabricius as a precursor in showing the true position of the lens (A.D. 1600), a host of observers rapidly built up the basis of the anatomical scheme as we know it today.
Fallopius rediscovered the greater curvature of the cornea and
stressed the difference in structure as between the cornea and sclera. A clearer view of the capsule of the lens and a description of the hyaloid membrane likewise came from him. He differed from Vesalius in regarding the ciliary body
as a membrane, and held it to be a ligament binding the lens to the choroid. Incidentally, he also disproved the existence of the retractor bulbi in man. Ruysch, who studies the vascular structure of the choroid, is also
responsible for showing the existence of circular muscle fibres in the iris. Briggs, who is remembered for his demonstration of the existence of the optic papilla (regarded by him as a projection, as its name implies), showed that the
retina extended up to the ciliary "ligament." What the 16th century began falteringly was well done in the 17th. A comparison of two reproduction showing the state of anatomical knowledge towards the beginning and the end of the 17th
century is of interest (Figure 5 and 6).

Figure 5. Illustration from Scheiner (1575-1650)
Figure 6. Illustration from Molinetti (?-1673)
The finer methods of anatomical study were first used in that century; Ruysch employed injected preparations for the study of the vascular system of the eye; Malpighi used the hand-lens and Leeuwenhoek made the first observations with the
microscope; but it was left for the succeeding century to introduce the study of the frozen eye, an innovation due to Petit. The combination of these methods led to the rise of a detailed anatomy, for the bold outlines were by now firmly
established. Petit was the first to attempt measurements of the components of the eye. Priority in the description of Descemet's membrane was the subject of a word dispute between Demours and Descemet, but its first indication is really to
be found in Duddell.
In studying the constitution of the lens, Morgagni found fluid between the capsule and the lens fibres. This fluid was held to nourish the lens - a mistaken notion but one which, at any rate, was an advance on the
belief that the lens and cornea contained vasa serosa, which possessed the property of impermeability to red blood cells. To the anatomy of this period belongs the description of the spaces of Fontana, as also the discovery by
Demours of the canal of Petit, so named by him, the Zonula of Zinn commemorates the name of an observer who also contributed studies on the blood-vessels around the entry of the optic nerve (circulus arteriosus of Zinn) and on the
action of the ciliary body.
The presence of muscle fibres in the ciliary body was a matter of much discussion; some held with Morgagni that they existed and affected accommodation, others with Zinn, that they were non-existent. Similarly contraction and dilatation
of the pupil were explained on the conflicting view that different degrees of congestion of the vessels of the iris produced changes in the size of the pupil.
It is noteworthy that even at this late stage some gross points were still unsettled. Though Petit in 1728 had clearly demonstrated the posterior chamber, its existence was being questioned down to 1855 and it was not until the work of
Helmholtz, Henle and Arlt that this question was finally settled.
Whilst by the end of the 18th century the uveal tract had been fairly well described, the retina was barely recognized, for the day of cellular anatomy had not yet come. At the turn of the century Buzzi, Sömmering and Reil described the
macula lutea. The additions to our knowledge of the anatomy of the eye during the 19th century are largely the history of the consequences of the introduction of the compound microscope and the rise of the cellular theory.
The advances recorded during the earlier part of the 19th century, before the introduction of the microscope, are typified by the description of Jacob's membrane. Jacob described a serious layer in the eye, lying between the retina and
the choroid; this ultimately came to be regarded as a constituent part of the retina, which was held to consist of three layers, a limiting layer, a nervous layer — the retina proper — and Jacob's membrane. Jacob's membrane is indeed
nothing else than the rods and cones of modern histology. To this period belongs also the discovery of the canal of Schlemm.
The compound microscope opened a new realm of observation, and the realization of the significance of the new facts which were rapidly gathered, culminated in Schwann's theory that all living matter consists of cells. As early as 1722
Leeuwenhoek had noted the rods and cones of the retina, but their existence had to be rediscovered in 1834 by Treviranus. And just as the retina was gradually being recognized, so other tissues were studies by the new microscopic methods.
In a few brilliant years of intense work.
The nature of vision has been the subject of much speculation since the earliest days of systematized knowledge. To the natural philosophers of pre-Hippocratic days, vision was the result of information gathered by antennae-like
rays emitted by the eye; these rays on striking an object were deflected back to the eye, conveying information of the outer world. Such information would in turn be transmitted along the hollow tube connecting the eye with the brain. This
view, modified in one form or other, persisted in clinical ophthalmology, though not without challenge, till the beginning of the 17th century. Whilst the modifications constitute the history of the development of ocular physiology, the
challenges were merely brilliant asides.
The modifications that this theory underwent are essentially few. Plato held that in addition to the visual substance that emerges from the eye to gather information, there was
another factor — rays from the objects seen, which blend with those of the eye and thus produce vision. Alexandrian anatomists fixed the seat of vision in the lens, a view that Galen elaborated when he conceived the retina lining the
posterior aspect of the lens as a mirror in which the object is reflected and thence transmitted along the optic nerve to the brain.
A radical break from these views were those of atomists who conceived vision as the result of small particles constantly detaching themselves from objects and flying in all direction, including the eye. Aristotle likewise
approached the modern conception when he insisted that things are seen by influences emanating from them, rather than from rays emerging from the eye. But whilst speculation was rife, actual observation was not altogether wanting. Amongst
the Alexandrians, Ptolemy wrote a treatise on light; holding with his contemporaries that objects are seen by rays emerging from the eye, he taught that distance is judged by the length of the emergent rays, position by their direction, and
size by the angle rays subtend on striking an object. He recognized binocular vision and diplopia, even to the extent of describing the crossed and uncrossed varieties of double vision.
The nature of the visual spirits that produce vision was defined by Galen as pneuma; the pneuma, derived from the brain, fills the space in front of the iris, dilates the pupil and surrounds the lens. Short sight
resulted from weakness of the visual spirit; though it passes through the pupil and emerges from the eye it fails to reach an object in the distance. A later writer (Alexander of Aphrodosias, in the 3rd century), argued that the phosphene
seen on sustaining a blow on the eye was the result of the pneuma becoming inflamed.
The Arabian renaissance brought uneasy stirrings against the traditional view of vision as the result of energy emanating from the eye. Ar-Razi compiled a monograph: "On the nature of vision: wherein is shown that the Eyes are
not Radiators of light". But it was not till Alhazen (Ibn al-Haitam), in the 11th century, that a valid challenge emerged. Basing himself on the geometry and physics of his day he solved a number of optical problems, conclusively
establishing the view that objects are seen by rays passing from them towards the eye and not in the reverse direction as was believed. With Alhazen begins not only modern physiological optics but modern optics too, and during the Western
Middle Ages Robert Grosseteste, Roger Bacon, John de Peckham and Vitello contributed to the newer optics.
The more substantial optics that thus emerged had little effect on ophthalmic physiology. The gulf between the academically minded physicists and the itinerant oculists of the Middle Ages was too vast to be easily bridged, and
even to the physicians the newer optics percolated but slowly. Maurolycus, Leonardo da Vinci, Plater and Porta haltingly reached towards the conception of a camera obscura. Porta's statement is worth quoting, both for its formulation
of the newer view on the nature of vision and for its retention of the fallacious physiology of Galen: "As objects illuminated by the sun send their light through a narrow hole in the window-shutter upon a paper placed opposite, exactly so
does light, passing through the hole of the pupil, produce images of objects looked at upon the crystalline lens." That the retina and not the lens was the receiving plate of the eye was held by Plater, but till Kepler were his views
harmonized with those of Porta.

One of Leonardo da Vinci's notebooks
In Leonardo da Vinci's notebooks there are many sketches relating to the questions of optic and vision.
However, his understandings were not always accurate. The sketches here show the vertical sections through the scalp and the eye; the course of the optic nerve is mistakenly shown to be connected with the anterior ventricle.
Kepler's work is the consummation of that of Alhazen. With Kepler the eye becomes an optical apparatus obeying the laws indicated by the Arabian. The camera obscura conception becomes complete- the retina is the receiving plate,
the lens and cornea are refracting media. With an understanding of the optical properties of the eye came the appreciation of the significance of myopia and the rational use of glasses.
A number of problems pressed for
solution as a result of Kepler's work. The precise optics involved acceptance of an inverted image on the retina. That this indeed occurs was shown shortly afterwards by the Jesuit Father Scheiner in an experiment in which a windown was
made in the posterior pole of animal eye. Scheniner was also responsible for measuring the indices of refraction of the components of the eye; he measured the radius of curvature of the cornea by the simple expedient of placing glass
spheres of known curvature alongside the cornea and finding which sphere gave an image of equal size to the image of a windown seen on the cornea. But apart from the accurate physical measurements that were being undertaken, the conception
of the eye as an optical instrument precipitated the problem of accommodation. Obviously if the eye could register impressions of objects both near and far, it was a dynamic and not a static optical apparatus. Accommodation was thus
recognized as a property of the healthy eye, and the problem of accommodation formulated by Kepler was to baffle physiologists for well over two centuries.
Kepler himself held that accommodation was affected by the ciliary processes either through a change in the form of the eye, the antero-posterior diameter becoming shorter and the horizontal diameter wider, thus bringing the
retina nearer to the lens, or alternatively that the lens was moved from its position. Further possibilities were advanced by other observers. Descartes held that in addition to change in the length of the eye, which he regarded as due to
the action of the extraocular muscles, there were also changes in the form of the lens, induced by the ciliary processes. His views as to changes in the form of the lens were supported by William Briggs. Other (de la Hire, Haller) sought to
explain accommodation on the basis of Scheiner's observation that the pupil contracts during accommodation; it was held that the elimination of diffusion circles by contraction of the pupil would account for the clear vision for near
objects in accommodation — a view supported by the fact that objects are seen more clearly through a pin-hole. Changes in the curvature of the cornea were held responsible by Albinus and Ramsden. Supporting the theory that accommodation is
produced by changes in the curvature of the lens, Jurin advanced the hypothesis that such changes were brought about by displacement of the Morgagnian fluid of the lens; whilst independent contractility of the lens was postulated amongst
others by Leeuwenhoek and Thomas Young, who regarded the lens as a muscular structure.
Young's laborious investigation on the structure of the lens failed to demonstrate nerve fibres in it, though his "full conviction of their existence"
was unshaken. in spite of his faulty anatomy Young nevertheless solved the problem as ot the seat of accommodation by experiments on his own eyes. He dismissed the cornea from consideration by finding that his accommodation was unaffected when he eliminated the cornea optically. This he did by using a forerunner of the modern contact glass - a weak objective lens of microscope placed before the eye with water between the
objective and the cornea. Young, who had very prominent eye, further disproved that the eye elongates during accommodation by clamping his own eye between two rings, one placed on the anterior surface of the eye, turned inwards as much as
possible, and the other, the ring of a small key, thrust on the external side between the orbit and the globe till the phosphened reached the fovea. Thus clamped, the eye could not elongate during accommodation, and as this was not
abolished and as furthermore the size of the phosphene did not change during accommodation — as it would have done if the eye had elongated — he held that accommodation is independent of elongation. Young concluded in favour of regarding
changes in the surface of the lens rather that in its position as the responsible factor. As additional proof that the lens was the seat of accommodation he pointed to the fact, stressed before him by Porterfield, that in aphakia
accommodation is abolished. The mechanism whereby the lens surfaces changed he could not elucidate. The discovery of the ciliary muscle had to wait another fifty years, and it was left to Helmholtz by means of his phakoscope to demonstrate
the actual changes in the curvature of the lens and to describe the nature of accommodation. In doing so Helmholtz rescued Young's work from under a spate of theories which continued to flourish in spite of Young's demonstration of their
untenability.
Another consummation of the work of Alhazen came with Donders. The rather florid judgement of Hirschberg is not an exaggeration: "Donders' work is of that wonderful clearness that is seen in alpine scene under a marine blue
sky; each chapter is like a self-contained valley: the writing is polished and therefore so penetrating and permanent." Original observations are not lacking, but these of themselves would not place Donders in the forefront amongst the
immortals. Much the most significant thing is the critical analysis which pervades his work. Before Donders refractive errors were classified according to the correcting lens required; myopia was the condition in which concave lenses were
needed, presbyopia in which convex lenses were required. The puzzling thing about ""presbyopia" was its occasional occurrence in young people — "old sight of young people." Many people before Donders had conceived of hypermetropia; many
too had realized that disturbances in accommodation could result in defective vision. It was however left to Donders to separate clearly errors of refraction from those of accommodation. It was he who introduced hypermetropia as the
antithesis of myopia, clearly separating it from presbyopia, thus demolishing the "old sight of young people."
The concept and the term emmetropia also came from him. Many years before Donders, Thomas Young had described astigmatism, but a mass of hazy notions on the subject awaited crystallization in Donders' writings.
Apart from clear classification, the clinical aspect of refractive errors was well elucidated. Donders introduced the classical formula for determining the range of accommodation; conceiving presbyopia as a diminution of the
power of accommodation he established the absolute, binocular and relative range of accommodation, and also showed that the correction of presbyopia relieves headache. Myopia was critically considered from analysis of thousands of cases,
and the problems it presented as to heredity, close work, ophthalmoscopic appearances, anatomy, symptoms and treatment were clearly brought out. The innovations since 1864 when Donders' classical Anomalies of Refraction and Accommodation
was published, had added or detracted little of material value, though the full benefit of this work could not be realized till the introduction of the shadow test by Cuigenet in 1873 and by the use of mydriatics. The new outlook that
Donders contributed to ophthalmology is well illustrated by the fate of "asthenopia" a term first introduced by Mackenzie in 1830. To Mackenzie, who regarded the symptoms as due to retinal exhaustion, the condition was of such serious
import that giving up work and long sea-voyages were considered appropriate treatment. Since Donders, asthenopia has come to stand for one of the minor ailments.
In the century following Kepler's, attention was being given to the fundamental physiology of the eye. Mariotte had already discovered the blind spot in 1668, and Briggs the optic papilla in 1676; Porterfield in 1759 showed
that the blind spot was indeed the entry of the optic nerve. Porterfield further insisted that the retina and not the crossroad, as Mariotte believed, was the essential organ of sight. Whilst attention was being given to after-images and
suggestion even advanced that they are the result of fatigue of the retina, these and allied problems were generally regarded as beyond explanation. Porterfield well expressed the contemporary attitude in a passage characteristic of his
century, "The connection betwixt our Ideas and the Motions excited in the Retina, Optic Nerves and Sensorium is unknown to us, and seems to depend entirely on the Will of God." Binocular vision, though Briggs had advanced the theory of
corresponding points, was likewise explained in terms of theology; to Porterfield it was a reflex act of the soul. It was not till the 19th century that progress in these fields of study became established.
Binocular vision began to become intelligible with the introduction of the stereoscope by Wheatstone and with the studies of David Brewster. Studies of the field of vision, though indicated by Thomas Young, did not begin
seriously till taken up by von Graefe, working with sheets of paper on which he had drawn radiating lines to act as meridians (1855). The work on colour vision by Helmholtz was likewise, a return to Thomas Young.
Ocular movements too had to wait till the 19th century for any intensive study. The work of Johan Muller led to the studies of Listing and to the formulation of Listing's law in 1857.
After Helmholtz had proved that not only the optic disc but also the optic tracts were insensitive to light, and Muller had shown that the layer of rods and cones was the recipient element, Weber (1852) drew attention to the
exclusive presence of cones at the macula and the formulated the theory that the cones alone are the light receiving elements.
Like all pathology, that of Hippocrates was the reflex of the prevailing philosophy. The Ionic school held that there were four elements: water, fire, earth and air, and that these gave to matter its four cardinal properties: moisture,
warmth, dryness and coldness. this was translated in terms of physiology as four cardinal humours: blood, mucus, yellow bile and black bile. Health resulted from the proper and proportionate admixture of these humours in the body: disease
implied a disturbed balance. Left to itself the disturbance ran through three stages — crudity, when the disturbance occurs, coction, when the body prepares to expel the disordered humours, and crisis, when that
process takes place. There were in addition seven injurious humours passing from the brain to the tissues, this constituting the catarrhal process. One humour passed into the nose and the two affected the eyes, one of these producing the
discharge in ophthalmias and the other affecting vision without producing an external discharge.

In ancient Greece, the healers and patients used mystical religious rites in the treatment of eye diseases. Eye votic gifts (offerings) were very common. Some of these were plea for health as in the picture on the right
which depicts
a boy with a lesion on the right eye and exophthalmos. The picture above is made of bronzed lead covered with silver; a gift to the gods as thanks for a cure of
the eyes.
from The Eye & its diseases in antiquity by A. Ry Andersen

This fanciful stuff apart, the Hippocratic school was responsible for some sound observations. They recognized not only the inflamed eye but such external conditions as could be appreciated without any detailed knowledge of
anatomy; they were acquainted with such things as chalazion, pterygium, ectropion, entropion, trichiasis, nystagmus and squint. Though no detailed clinical appreciation was achieved. it is characteristic of their powers of observation that
they recognized blindness following haemorrhage — a close approach tot he blindness from optic atrophy consequent on haematemesis and metrorrhagia.
Alexandrian ophthalmology, as preserved by the writings of Celsus, shows considerable
advance in the recognition of disease. A clear distinction is made between moist and dry ophthalmia (ophthalmia and xerophthalmia), and a good account of trachoma is given under the term aspritudo, the name trachoma not being
introduced till three centuries later by Severus. A number of additional external conditions, such as proptosis, and lagophthalmos, are also described, and much more definite information is given.
The ocular pathology of Galen marked but little progress. it was more systematized, and recognized eye disease as resulting from affections of (1) the crystalline body, the essential organ of sight; (2) the brain and visual nerve,
involving disturbances in the visual spirits proceeding from the brain along the visual nerve to the essential organ of sight; and (3) of other parts of the eye distinct form the essential organ of sight. Disease of the crystalline is shown
by glaucoma, the greenish discoloration being produced by drying of the of the lens; the condition is incurable, affecting as it does the essential organ of sight. Disease of the brain and visual nerve is shown typically by cataract, the
corrupt humour settling in front of the lens. Disease of other parts of the eye affects the pupil or the space between the pupil and the lens, the aqueous and pneuma being at fault.
In the succeeding centuries this doctrine became dogma. The Byzantine commentators added little of their own and the Arabians could not break away from the concept of ophthalmias and of corrupt humours settling in the eye, though their
clinicians were responsible for some remarkable observations. Thus Rhazes (Ar-Razi) recognized the pupil reaction to light, whilst Sams-addin described "headache of the pupil" — probably the first, though vague, recognition of acute
glaucoma, pannus too is first described in Arabian writings.
The weary process of commentaries upon commentaries dragged on even after the Renaissance. But little had been gained in the meantime except some clearer definition. The humoral theory of disease underlay the separation of blindness into
two varieties, gutta serena and gutta opaque. In the first the pupil was unclouded by the morbid humour, in the second it was affected. Gutta serena and suffusio nigra was sometimes used in contrast, but more frequently as synonymous with
glaucoma, blindness with a greenish pupil. That no real understanding underlay this classification is obvious enough.
The 17th century saw the overthrow of the theoretical basis of Galen's ophthalmology, but clinical ophthalmology hardly escaped from the framework of his theories and teaching. The new anatomy and physiological optics permeated but
slowly, and it was left to a few French workers in the succeeding century to evolve new clinical conceptions. The recognition of the seat of cataract was the opening of the chapter; this brought new views as to the nature of glaucoma. And
equally significant, even though it led to a blind alley, was the rise of a new orientation in the description of disease processes. What basis of purely anatomical description there was in Galen — descriptions such as pterygium and
hypopyon — were taken over, and attempts were made to describe the ophthalmias in terms of aetiology. The iatrophysicists had too evanescent an influence to affect ophthalmology, but the succeeding iatrochemical school described ocular
disease in terms of chemical disturbances, or diatheses. Thus arose conceptions like catarrhal, rheumatic, arthritic, scrofulous, gouty, haemorrhoidal and cancerous ophthalmia. Though this led to much clinical observation, and the
incidental isolation of such things as gonorrhoeal ophthalmia, ultimately this activity produced a stranglehold of fantastic descriptions with no basis in fact. It reached its climax with Beer's classical text-book published at the
beginning of the succeeding century. During this process of evolution the ophthalmias came to be recognized as consisting of external and internal varieties, the internal varieties following the same sort of classification as had already
been applied to the external ophthalmias.
It remained for the 19th century to demolish all this. And whilst in the 18th century the pioneer work was done almost exclusively in France, the trend of newer thought came from England by the publication in 1808-18 of Wardrop's
Essays on the Morbid Anatomy of the Human Eye. In describing disease Wardrop broke away from hypothesis, and in the true Hippocratic manner concentrated on observation and fact. Though he began before the compound microscope had come
into use, he dealt with ocular lesions on a strictly anatomical basis, speaking of inflammation of the cornea, iris, choroid and so on. He introduced the term keratitis, though the credit for the term iritis belongs to Schmidt, who used it
in 1801. Wardrop's efforts attracted rather more attention in France than in his native country, for English ophthalmology was dominated by Beer; and Mackenzie, with his classical text-book of 1830, helped to perpetuate the system of Beer
and of other Teutonic writers. Yet the anatomical classification was slowly gaining round, some of Wardrop's excesses naturally being modified in the process. Thus hyalitis, descemetitis, and capsulitis came to be dropped. In 1836 Schindler
described fully several forms of keratitis, including interstitial keratitis. Equally significant was the slow disintegration of the conception of internal ophthalmia. The term cyclitis came to be introduced in 1844 (Tavignot), and though
such monstrosities as aquo-capsulitis and cristallino-capsulitis were introduced and lingered for some time, the generalization of all intra-ocular disease as one had become a matter of the past.
All though this years progress in observation was also being made. The charlatan Chevalier Taylor described keratoconus, though preceded in this by Duddel; Beer corrected Scarpa's error in regarding pannus as a similar condition to
pterygium, whilst a few years later Fabini (1830) drew attention tot he fact that pannus often follows trachoma. Blindness in association with nephritis was observed even before the classical description by Bright.
The complete demolition of internal ophthalmia and of the fantastic aetiology of disease could not however be achieved till the coming of the ophthalmoscope for the one and the rise of bacteriology for the other.
The ophthalmoscope incidentally led to the recognition of the nature of glaucoma, a last remnant fo the internal ophthalmias. Yet such names as renal retinitis for a frankly non-inflammatory lesion are monuments to the influence of the
older conception of ophthalmia. Bacteriology, whilst overwhelming much aetiological fantasy, established definitely such things as the gonorrhoeal nature of ophthalmia of the newborn, which was well described and recognized as of venereal
origin by Ware in 1795. Ophthalmia neonatorum had variously been explained as due to contact with leucorrhoeic discharge, as the result of compression of the infant's head, as the effect of baptismal water, whilst Mackenzie saw it as the
result of the soap with which the newborn infant was washed getting into its eyes.
  
Glioma of the retina showing the front and side views in the above pictures.
The picture on the right is the same patient post-operative (1885).
In the first authentic document on the subject, the writings of Celsus, there is a complete teaching on the pathology and treatment of cataract. The preceding Hippocratic writings are silent on the
subject, so that the Alexandrian school must have developed the teaching to the advanced level seen in Celsus. What exactly the Alexandrians did and where they found the basis for their studies, is a matter of conjecture. It is possible
that the operation for depression was known in India since early days, but the evidence that it was known in Egypt and Babylon is more than doubtful. Celsus' account of cataract and its treatment was indeed the teaching that persisted till
the 18th century with hardly any modification. The sudden eruption of a complete system of pathology and treatment from out of a historical void is but one of the many strange things in the history of cataract.
Cataract as a name is of comparatively recent origin. It arose out of medieval Latin translations of Arabic writings and was a sort of shorthand term for expressing the pathology of the condition
— humour that flowed down into the eye.
The older Latin name was suffusio and the Greek name, hypochyma, both having the same humoral implication; but these names were not revived to any extent when, with the Renaissance, men turned from translations from the Arabic
to the original classical sources.
Suffusio with Celsus stood for that form of blindness which could be relieved, as opposed to glaucoma which was a form of incurable blindness. In suffusion corrupt, inspissated humour collected in the locus vacuus between
the pupil and the lens, thus obstructing the visual spirits. By clearing this empty space vision could be restored. The obstruction caused by the suffusio could be removed in the early stages by medicinal treatment, but when fully
formed only by operative displacement into a part of the eye other than the front of the lens. The operation involved entering a sharp, but not too slender needle into the eye and when resistance was felt on touching the suffusio,
this structure was gently worked down away from the pupil. If it did not stay down the suffusio had to be broken up in pieces and these fragments were then depressed. Celsus gives a detailed account of the pre- and post-operative
treatment. Incidentally, a later Roman writer attributed the development of this operation to the casual observation that vision was restored to a goat, blind from cataract, when it ran its eye on to a thorn.

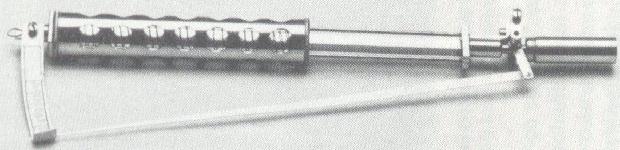
A set of couching needles.
The conception of cataract as inspissated humour in front of the lens persisted with Galen, in whose anatomy there was no locus vacuus. During Arabian times the conception became even more firmly rooted and the central
position of the lens in the anatomy of Vesalius is evidence of the firmness with which the belief was held. The epoch-making work of Kepler and his forerunners in dethroning the lens from its position as the essential organ of vision had no
immediate result on the teaching as to the nature of cataract. At about the middle of the 17th century more than one observer began to question whether cataract was not indeed an affection of the lens, but the rooted belief that glaucoma
was due to drying of the lens was a great obstacle to the resolution of these questions and doubts. Characteristic of these doubts is the observation by Dechales that the reason why strong convex lenses are needed by patients operated on
for cataract must be that the secretion destroys the spherical shape of the lens. By actual demonstration of an opaque lens in cataract, Rolfinck in 1656 crystallized a considerable amount of discussion and teaching by both physicists and
oculists. About thirty years later Maître-Jan noted that it was not a thin membrane but a thick rounded body that was displaced when on two occasions he chanced to displace the cataract into the anterior chamber instead of into the vitreous.
e further had the opportunity of examining the eyes of patients whose cataracts he had couched and found that it was the lens itself that was displaced. He concluded that cataract and glaucoma were indeed one and the same disease, but the
one was curable and the other not.

Couching (depression of the lens)
in the late 16th century.
These observations passed unnoted. When Brisseau, a young man at the beginning of his career, rediscovered in 1705 all this for himself, his friend and teacher Duverney advised him
against publication, if he did not wish to jeopardize his future. However, his findings went forward to the Académie Royale des Sciences, through the intermediary of a member of it, only to be told that the views expounded therein
had made but little impression. Brisseau had nevertheless succeeded in raising a controversy — a thing in which his predecessors had failed. Maître-Jan came forward with his own proofs as the truth of the new conception, and Brisseau
himself advanced further proof. De la Hire and Mery were prominent in the opposition, whilst Petit supported Brisseau. However, in searching for conclusive evidence against Brisseau, Mery convinced himself of the error of his own views and
came out in the Academy strongly in favour of the new teaching. Indeed in the Academy the battle was soon won, but for years the repercussions distracted the rest of Europe. Boerhaave, Morgagni, Valsalva and Cheselden were amongst the
supporters of the new school, whilst prominent amongst distinguished opponents was that brilliant charlatan, Thomas Woolhouse.
The acceptance of the new pathology precipitated acutely the problem of glaucoma, for glaucoma was acutely the problem of glaucoma, for glaucoma was held to be a disease of the lens. It also forced attention to such conditions as
obscured the pupil and were not cataract. It thus involved a new pathology as to the causes and treatment of blindness.
Hardly had the furore caused by this controversy died down before another storm broke which was destined to last throughout the second half of the 18th century and to be prolonged well into the 19th. Brisseau did in 1743b. Five years
later Daviel published his account of extraction of the lens.
The radical treatment of cataract as practised today is essentially the method of Daviel. But previous attempts at radical treatment were not wanting. Indeed there are puzzling passages in the older writers which would lead one to
believe that extraction had some transient vogue in ancient days. There is the bleak passage in Galen which speaks of some who, instead of displacing the cataract to a site where it is less troublesome than in front of the lens, "have
attempted to extract it, as I shall show in the book dealing with operation." This book is lost and the later Greek writers do not refer to the operation. Roundabout information comes from Arabian sources. Salah-ad-din reports Razi as
saying that according to Antyllos some divide the lower part of the pupil and extract the cataract, the procedure being possible only with thin cataracts, as with thick cataracts the humour (aqueous) also escapes.
These references to extraction in all probability implied some form of evacuation. A much more significant attempt at the radical removal of the cataract is due to the Arabian, Ammar, who elaborated the operation of suction. The
introduction of a glass tube through a corneal incision for removing cataract is also referred to in the passage "according to Antyllos." Arabian practitioners before Ammar certainly practised it, but it was left to Ammar to devise a hollow
needle introduced through the sclera, thus avoiding an incision into the anterior chamber and consequent loss of aqueous, which was regarded as a calamity. Western Caliphate and in Christendom. In the East it found a readier reception. In
Western Europe the operation had to be rediscovered during the last century.
Surgical treatment of cataract at the time of Daviel was therefore confined to depression. Breaking up the lens piecemeal, to induce depression in such cases where the lens would not stay down, was a course adopted only as a matter of
necessity. Daviel's cataract operation was therefore as marked an innovation in treatment as the work of Maître-Jan and Brisseau had been in pathology.
Before Daviel the possibility of extraction was "in the air." When Mery recognized the truth of Brisseau's work he also saw that it might be possible to extract the opaque lens by an incision into the eye. The lens was actually extracted
by St. Yves in 1722, but it was extraction of a lens which had become displaced into the anterior chamber during an attempt at depression. Piecemeal removal of a broken-up lens, particles of which had floated into the anterior chamber, was
also carried out by Petit; and it was a similar unplanned emergency procedure that started Daviel on his planned extraction. What had been forced on him by accident and, incidentally, had proved utterly unsuccessful, he repeated
deliberately in a second case — deliberately making an opening through the cornea and removing the lens piecemeal. Actual extraction of the lens en masse was forced on him in a case in which he failed to couch the cataract. He then "decided
to open the lower portion of the cornea in order to get my needle the more effectively into the posterior chamber". A year later (1748) he published his account, but it was some years before he finally decided in favour of extraction to the
exclusion of depression.
Daviel's operation consisted of a corneal incision near the limbus below, made by puncture with a sharp curved needle, enlargement of this puncture to the right and left with a blunt curved needle, and completion of the incision to the
right and left with curved, convex scissors; the incision having been made, a spatula was introduced into the eye, and while it held the cornea away from the lens, the sharp needle was used for opening the capsule; the spatula was next
passed between the iris and lens to free any adhesions; gentle pressure to dislodge the cataract completed the operation (see picture below).

Daviel's method of cataract extraction
The operation was taken up enthusiastically — but only for a brief space. Everywhere influential support for the older operation became consolidated, and new methods for couching were developed. During the hundred years in
which Daviel's operation was on trial many modifications of an ephemeral vogue were introduced. The complicated incision practised by Daviel soon enough gave way to a single incision by a knife, special patterns being introduced by almost
every operator. At an early stage incision at the upper limbus was proposed, but this gave way to a modified incision lower down. Other modifications aimed at different varieties of corneal incision, the variations ranging from
semi-circular to triangular. To obviate suppuration and promote better healing scleral incisions were advocated. This was partly the underlying principle of von Graefe's linear incision, an operation that was soon given up because of
cyclitis and sympathetic ophthalmia which so frequently followed. Mooren's preliminary iridectomy, introduced in 1864, constitutes the one generally accepted radical modification that Daviel's operation has undergone during its career of
nearly two centuries.
The term glaucoma goes back to hippocratic times. Its meaning is disputed; generally accepted to signify greenish — like the colour of sea water — Hirschberg has shown that it is much more likely to mean bluish. It would appear that in
Hippocratic writings hypochyma and glaucosis were synonyms, and both vaguely referred to cataract. It is only with later Greek writers that a distinction was made between the two, glaucoma becoming the incurable condition as
opposed to hypochyma which was curable, though not always so. Glaucoma which came also to stand for an affection of the lens itself, as opposed to cataract, which was a perverted humour in front of the lens. It is not at all unlikely that
the term was applied indiscriminately to all blindness not considered as cataract and in which the pupil changed its colour. Absolute glaucoma with its "green cataract", as well as pupillary exudates, were probably included. Whatever else
it may have stood for, it certainly did not stand for chronic glaucoma of today, for in this, as well as in the bulk of acute glaucoma, the discoloration of the pupil is not a striking feature. In any case it would only be the terminal
stage of chronic glaucoma that would be recognized and this no doubt passed as amblyopia, amaurosis or, in later day as suffusio nigra or gutta serena.
Glaucoma, in antiquity, therefore hardly stood for any definite entity. But the term
created a problem in pathology when Brisseau showed that cataract was a disorder of the lens itself. Some, like Maître-Jan were content to let both diseases reside in the lens; others, like Brisseau, monopolized the lens for cataract and
satisfied themselves that glaucoma was an affection of the vitreous, a view that led to much anatomical work to show what exactly the changes in the vitreous were. Vitreous fluidity, vitreous floaters and all sorts of vitreous abnormalities
were brought forward as evidence for that view, and the discussions on the subject still persisted towards the middle of the last century. In these discussions other tissues were incriminated. Mackenzie, amongst others, blamed varicosity of
the choroid.
All these discussions were of necessity futile, for they centred round a word rather than round a pathological entity. The essential feature of glaucoma - hypertension - was not not generally recognized till about 1840, and even so,
recognition only extended to acute glaucoma and absolute glaucoma. It was in fact a new entity that was being built up — a disease in which the cardinal sign was increased tension, and in which the name glaucoma had come to be a
meaningless label. The problem was no longer why the pupil was discoloured but why the tension was increased.
The first clear recognition of absolute glaucoma came with Rikchard Banister in 1622. Discussing the differential diagnosis between curable cataract and incurable gutta serena in which "the humour settled in the hollow nerves, be
growne to any solid or hard substance, it is not possible to be cured" he gives foure wayes," one which is "if one feele the Eye by rubbing upon the Eie-lids, that the Eye be growne more solid and hard than naturally it should be." The three
other tests were no different from those in common use at that time for determining the curability of cataract. Banister's tetrad — long duration, no perception of light, increased hardness and no dilatation of the pupil on bandaging the
sound eye - is a passable account of absolute glaucoma. His teaching, however failed to attract any attention. Hardness of the eye is next found in the literature a hundred and twenty years later, in J.Z.Platner, with nothing like
Banister's completeness. At the beginning of the 19th century it was rediscovered; it appears in a number of books at about 1820, and in Mackenzie's classical text-book of 1830 it is given definitely in the differential diagnosis between
glaucomatous amaurosis and cataract
Acute glaucoma, though not under that name, has a more considerable antiquity. The Arabian Sams-ad-din recognized it as a distinct entity in the amorphous mass of ophthalmias. He described under "Migraine of the eye, also known as
Headache of the pupil" a condition in which there is a deep-seated pain in the eye associated with hemicrania and dullness of the humours; the condition is sometimes followed by cataract and dilatation of the pupil; if it becomes chronic,
tenseness of the eye and poor vision supervene. This conception of a distinct disease does not, however, seem to have prospered. Though tentative attempts at the recognition of acute glaucoma were made by several writers in the 18th century,
it is not till 1813 that really convincing description occurs — an account by Beer. A form of iritis is differentiated from the other varieties by its distinctive symptoms and in that it ends in blindness, a greenish hue (glaucoma), a
dilated pupil and cataract — a tolerable description of the terminal stage of neglected acute glaucoma, even though the cardinal sign of hypertension is mission. In his ambitious attempt to describe eye conditions on a basis of causation,
Beer named this acute condition as iritis of gouty origin. Rainbow colours and hardness of the eye in a condition termed glaucoma appear five years later in a description by Demours. Subsequent publication speak of arthritic iris (and
ophthalmitis), as well as glaucoma, in describing conditions which appear to have been the same, apart from the presence of the greenish pupil reflex in the latter. The first to recognized that these two conditions were identical was Sir
William Lawrence; he considered glaucoma " to be merely a chronic form of the same inflammation as the arthritic inflammation affecting the posterior coats of the eye". It was also he who introduced the term of acute glaucoma (1829).
Lawrence did not link up acute glaucoma with what we now call chronic glaucoma, but with what now passes as absolute glaucoma — their link being not hypertension but the greenish discoloration. It was only when the ophthalmoscope had
revealed cupping of the disc that hypertension as the essential feature of glaucoma was finally realized. Even so, von Graefe in 1857 missed chronic glaucoma; he speaks of the acute, chronic (ie, absolute), and secondary glaucoma and of
amaurosis with excavation of the disc. Not till Donders recognized this last group as glaucoma simplex was the unifying conception achieved, a teaching that gained greatly from Bowman's simple numerical notation in recording the findings of
digital measurement of tension.
When the older writers spoke of the incurablitiy of glaucoma, they were right not only by their standards but by our own, for the condition they discussed was absolute glaucoma. Acute glaucoma, in contra-distinction to chronic glaucoma,
only emerged after 1830, and that too must have been incurable, for only very severe attacks would be recognized as glaucoma and the treatment would not improve matters, for it consisted of the same as for other forms of iritis. Till 1857,
when von Graefe introduced iridectomy for acute glaucoma, the diagnosis was indeed tantamount to a sentence of blindness, for even relief from miotic was unknown till about 1875. Not infrequently matters must have been made worse by
treatment for belladonna was used.
Iridectomy for acute glaucoma received the same mixed reception as every great innovation, and not altogether without reason. The rationale of the operation was then rather vague. Von Graefe was led to the operation in the belief that
staphylomata of the cornea regressed after iridectomy, presumably because of lowering of tension. To not a few surgeons operative interference meant adding trauma to an already markedly diseased eye. Feeling ran high and the discussions in
the subject were by no means free from acrimonious tendencies. When the collective experience of the profession clearly established the value of the operation, discussion ranged as to its mode of action. To some the favourable results were
caused by a filtering scar induced by the iridectomy, and this led to the various sclerectomies having filtration as their object.
The cause of the increased intra-ocular pressure was seen by von Graefe in a serious choroiditis increasing the watery contents of the eye. To Donders it was due to an increased secretion of the choroid. Stellwag regarded it as the
result of increased pressure in the ocular circulation, whilst Priestley Smith stressed faulty excretion rather than secretion, the immediate cause being abnormalities in the angle of the anterior chamber.
Tonometers through the ages

Donders' tonometer (1868)
|

von Graefe's tonometer (1862)
|

Snellen's tonometer (1900)
|
Seeuwen's tonometer (1901)
|
Captain Cook found, in a previous unknown Australian island, a woman rubbing with a wooden stick the everted eyelids of a child. This primitive method of treating roughness of the palpebral conjunctiva seems to have a remote antiquity, and
is one of the few procedures of Hippocratic ophthalmology that has persisted. Friction of the everted lid was applied by means of rough wool wrapped round a wooden spindle, the process being kept up till a thin sanguineous fluid exuded.
This treatment was followed by local applications, generally containing copper.
Of the more ambitious systems of treatment based on Hippocratic pathology with its crudity, coction and crisis of humours led to inactivity when it did not
lead to drastic interference. In acute diseases of the eye, local remedies were avoided, and reliance placed entirely on measures influencing the humoral changes. Restriction in diet and hot foot-baths were amongst the most common, but
every means that would draw the morbid humour away from the eye — irritant gargles, cupping, venesection, cauterization of the blood-vessels in the neighbourhood of the eye, multiple incisions going down to the bone, and even trephining of
the skull to evacuate the humours — was employed. For chronic conditions, local applications containing ingredients well recognized in the more ancient civilization of Egypt were freely used — metals and spices as well as human milk.
Alexandrian therapeutics advanced greatly on this. Local treatment for acute conditions was not only recognized but highly developed, the means employed being collyria. Unlike the modern application, the collyrium was a solid medication,
made up in cakes of which gum was the basis. A fragment of a cake was dissolved in water, oil, milk of woman, urine, bile or saliva, before use. There was an endless number of these preparations, and the secret of their composition was
jealously guarded. Crude lettering embossed by metal or stone stamps, of which many have been recovered in excavations, gave the name of the collyrium, fo the maker, and indications for its use. The polypharmacy of the Romans is well
reflected in the composition of such collyria, the ingredients of which have been recorder. The collyrium of Hermon is reported by Celsus as containing no less than 21 substances, and the multitude of collyria recommended by him for
different conditions throws an interesting sidelight on this aspect of treatment.
In addition to collyria, the Hippocratic methods of treatment were also pursued. But it was the surgery of the period that constituted a real advance. As elaborated by Galen and his commentators it supplied a rather wide range of
operative treatment. Procedures for entropion and trichiasis were perfected; and an approach to the modern method of treating ectropion was made by Antyllos, as recorded by Paulus Aegineta: a triangular piece was excised from throughout the
whole thickness of the lid. Operations were also evolved for lagophthlamos, tumours of the lids, "aegylops" (swelling at the inner angle), ankyloblepharon, symblepharon, pterygium and panophthalmitis. Rather complicated sutures for the cure
of staphyloma of the cornea with or without resection were described by successive writers form Celsus onwards, whilst for hypopyon incision of the cornea and paracentesis were described by Galen, who also records that a certain Justus
cures hypopyon by shaking the patient's head. That the Romans had a full theory and practice of cataract has already been mentioned.
After Galen superstition began to creep back into therapeutics, and with it revivals of Egyptian and Babylonian treatment by meconium faeces and similar substance. Amulets, charms and invocations figure largely in Aetius and his
successors. Invoking the Deity was a usual introduction in the Arabian writings which, however, are not devoid of useful innovations, suction for cataract and peritomy in pannus being the most significant.
Astrology and its sister-study of herbs added encumbrances to the load of therapeutic measures under which ophthalmology was labouring. Towards the end of the 16th century Georg Bartisch, the father of German ophthalmology, in the first
book on ophthalmology that appeared in the vernacular, devoted chapters to sorcery, white magic and black magic, though it is fair to add that Guillemeau's book — in French — appearing two years later (1585) is not disfigured in this
manner. Easily the most crowning achievement in therapeutics during these long years of stagnation was the introduction of spectacles towards the end of the 13th century.
It was Bartisch who was responsible for the first surgical innovation that came with the Renaissance, by describing complete excision of the eye. Nearly 50 years later (1627) Fabry employed the magnet for removing a foreign body from the
eye, but this procedure received no general consideration till well into the 19th century. The 17th century was indeed sterile in the field of treatment. It was left to the 18th century to introduce three epoch-making operations — two
concerned exclusively with cataract, and the third very largely with it. Early in that century Petit, basing himself on the new anatomy of cataract, described breaking up the lens in soft cataract and leaving it to absorb instead of
attempting depression; and the middle of the century saw Daviel's work. But an entirely new innovation, and the opening of a chapter to which the succeeding century added greatly, was the operation for artificial pupil introduced by
Cheselden (1729).
Cheselden's operation had for its object the making of an opening in the iris by a needle introduced through the sclera in cases where the pupil was blocked either congenitally, after inflammation, or after couching for cataract. To a
generation which did not know of asepsis and of atropine in the treatment of the almost inevitable post-operative inflammation, the significance of the operation loomed larger than it does to us. Yet Cheselden's operation was ill-adapted to
the purpose it set out to serve. Performed in eyes in which the lens was in situ, it caused traumatic cataract. Chelselden's method of introducing the needle through the sclera frequently involved injury to the ciliary body; and, most
significant of all, the tear produced by a mere puncture was of transient value in most cases, any opening made contracting down or being filled with exudate before long. Attempts at improving the operation began with Sharp who, in 1740,
proposed transfixing cornea and iris by one incision across the anterior chamber. Other modifications aimed at cruciform incisions and at division of the sphincter at the pupillary margin. But the operation gradually fell into disrepute and
oblivion. In 1801 it was hailed as a new operation when Demours re-introduced it.
Cheselden's operation nevertheless opened a new chapter in the surgery of the iris. The modifications of his operation led to the development of iridectomy by Joseph Beer in 1798. Though a number of modifications and a variety of
specially constructed instruments came on the heels of Beer's simple procedure — carried out through a corneal incision made by the Beer knife and completed by withdrawing the iris with forceps and abscising it — Beer's operation came to
stay. Intended like Cheselden's for the formation of an artificial pupil, it led in the second half of the 19th century to the glaucoma iridectomy of von Graefe, and to its successors.
If the 18th century was successful in opening up methods for the conquest of blindness due to lens opacity and occlusion of the pupil, the 19th century groped unsuccessfully for the relief of blindness from opaque cornea. During the 18th
century tentative attempts were made to resect opaque areas; Erasmus Darwin in 1795 trephined out such areas, hoping to obtain clear cornea on healing. Other attempts aimed at excising a scar and suturing clear cornea, and even at the
making of windows in the sclera. But the problem which attracted most attention during the first third of the century was complete transplantation of the cornea. Successful enough on rabbits, it failed in man; the lingering discussions on
the subject were revived by the suggestion (Nussabaum, 1856) that a small glass lens might be implanted in the cornea. This, too, led to disappointment; successful operation led to irritable eyes.
Closely allied to these attempts were the efforts to bring a clear part of the cornea into the line of vision. Optical iridectomy was but one of these; others aimed at iridectomy combined with the newly described operation of tenotomy,
to bring the eye into a central position. Tattooing of the cornea was revived by de Wecker in 1872, after a chequered career; it had been practised by Galen, condemned by Aetius, resurrected by Guy de Chauliac in the 14th century and once
again condemned by Maitre-Jan in the 18th century.
The 19th century perfected the operation of enucleation introduced by Bartisch, who incidentally had limited its indications to such massive proptosis that the eye was hideous and could not be concealed. Bonnet in 1841 and White Cooper
in 1856 introduced the method of operation as it is practised today, whilst evisceration and exenteration did not come till later.
Excision as a therapeutic measure in sympathetic ophthalmia was the achievement of the second half of the nineteenth century. Sympathetic ophthalmia was first clearly indicated by Duddell in 1729, in recording that he had seen many cases
in which both eyes were lost, though only one was originally injured. But it was not till nearly a hundred years later that any clear conception was developed. Demours did much in that direction, but it was Wardrop who drew attention to the
fact that veterinary surgeons destroy the injured eye of a horse with lime or a nail in order that the good eye may be save. Both the writings of Demours and of Wardrop appeared in 1818, and in both the term sympathetic involvement is
employed. The first comprehensive description appeared in the third edition of Mackenzie's textbook (1840), and thereafter the seriousness of the condition and its relationship to injuries and retained foreign bodies was well realized.
Wardrop had advocated incision into the cornea and removal of the lens and vitreous of the injured eye as a prophylactic measure, but it was left to Prichard, of Bristol, to introduce in 1851 excision for that purpose. Only after Critchett
had show, twelve years later, the ineffectiveness of excision once sympathetic inflammation had broken out, was the full value of Prichard's procedure fully appreciated. Thereafter excision rapidly replaced such methods of treatment as
division of the optic nerve, of the ciliary nerves and the operation of iridectomy advocated by von Graefe.
Another procedure that was perfected during the century was the magnet operation. Dixon in 1859 deliberately incised the eye to extract a magnetic foreign body, whilst McKeown in 1874 went further; he explored the eye with the tip of a
magnet introduced into the vitreous. Hirschberg a year later invented the electro-magnet.
The crowning achievement of the 19th century in ophthalmic surgery was, of course, the operative treatment of glaucoma. But it did much in plastic operations on the lids; and the introduction of asepsis and general anaesthesia was a much
a boon to ophthalmic surgery as to surgery in general. The introduction of cocaine in 1884 as a local anaesthetic had of course special significance for ophthalmology.
It was also left to the 19th century to give a clear lead in the treatment of squint and of lacrimal obstruction. Both conditions had indeed been noted in antiquity, bu the conceptions concerning their nature were of the vaguest.
Squint was the evil eye of mythology and primitive folklore. in Hippocratic writings the fact that it frequently affects parents and children is clearly recognized. An early attempt at treatment is recorded in Paulus Aegineta; this
consisted of wearing a mask with two perforations placed centrally before the eyes. It was argued that the squinting eye, finding vision obstructed by the mask, would assume a straight position. Fixing bright objects to the outer side of
the in-turning eye was likewise attempted; it was held that the attention which these objects excited would make the eye take up a normal position. Little progress was made on this till well-nigh the 19th century. Ambroise Pare, towards the
end of the 16th century, could only fall back on the method of Paulus. During the 18th century squint was regarded as the result ot malposition of the cornea or of tilting of the lens. But whilst orthodox practitioners could do nothing,
the itinerant Chevalier Taylor undoubtedly put squinting eyes straight. Apparently he had discovered the fact that division of the internal rectus would sometimes straighten the eye. Surrounding his activities with much pomp and mystery, he
probably performed subconjunctival tenotomies. At any rate there was always and admiring crowd to shout "a miracle." Much more significant was the work of Buffon. He recognized that the squinting eye generally had poorer vision than the
fellow eye, and held that this inequality would render objects confused. His treatment was to cover the good eye, or alternatively to place a convex lens in front of it, whilst the affected eye had a plane or concave lens "in proportion to
the strength or weakness of each eye."
It was well-nigh a hundred years after Taylor before surgical treatment of squint was to become common heritage. Tentatively suggested by Anthony White in 1827, and by others, the first successful operation — a myotomy — was performed
in 1839 by Dieffenbach. Numerous modifications have followed since his day. And just as Taylor was followed by Buffon, so the surgical treatment of Dieffenbach was followed by the optical treatment of Donders, who in his classical work of
1864 showed not only the existence of hypermetropia in squint, but the frequently unequal degree of it in the two eyes and also the disturbance of balance between accommodation and convergence in hypermetropes. The fusion theory of which
Javal was the main exponent, dates from about the same time.

Michelangelo's David, for centuries the epitome of male beauty,
has a flaw. He squints. The discovery was made during an
exercise to produce a digital version of all Michelangelo's
sculptures and buildings by scanning them with a laser. The
result shows the gaze directions of his eyes diverge.
This is shown clearly in the full frontal image of David's face, which cannot normally be seen because the sculpture is 16ft tall, stands on a pedestal, and is seen from below at an angle at which the face is obscured by the left hand. It is believed that Michelangelo did this on purpose, because it provided good profiles of David when seen from either side by optimising each eye for its appearance as seen from the side.
In the classic view of the statue, looking at the right side of the face, David gazes off to his left. The view of the left profile is seldom seen these days, because it would involve looking through the wall of the Galleria dell'Accademia in Florence, where the statue is displayed. In its original site outside the Palazzo Vecchio it would have been visible.
Lacrimal obstruction has a more prolonged and varied history. Though Galen knew the lacrimal glands, the canaliculi, and the drainage into the nose, the pathology of the lacrimal apparatus was ill understood. Under the term aegylops were
included all swellings at the inner canthus; and the treatment described by Celsus, Galen and their successors was drastic in the extreme; some form of incision down to the bone and the application of the red-hot cautery was the favourite
method. Among the Arabians, Avicenna may be regarded as a pioneer in treatment by probing on account of his suggestion to introduce into a lacrimal fistula probes carrying medications. The Renaissance brought accurate accounts of the
lacrimal apparatus by Vesalius and Fallopius, but it was left for Stahl in the 18th century to show that the aegylops of antiquity was not an affection of the soft tissue, but the consequence of lacrimal obstruction and inflammation.
Following this recognition, lacrimal affections were regarded as being either hydropsia — when regurgitation from the sac could be obtained — or ulcerative, when a lacrimal fistula was present. Anel in 1714 was a voice in the wilderness
when he evolved a treatment for lacrimal obstruction, in which probes with an olive eminence were passed into the sac through the upper punctum whilst an astringent lotion was injected through the lower punctum by a syringe, which, like
the probes, was devised by him and still bears his name.
A variety of modifications were evolved. Guidethreads, for the introduction of medications into the sac, incision into the sac and catheterization through the incision; retrograde
probing; and endless variety of probes; permanent implantation of tubes, were all suggested or tried at different times. Blizzard proposed the injection of metallic mercury, so that by its very weight it would clear a passage. By the
beginning of the 19th century Anel's procedure had fallen into oblivion, though search still continued for the perfect method. Various attempts at cauterizing the nasal duct by silver nitrate were tried, whilst sealing the puncta was
another procedure that had some vogue. It was Bowman who in 1853 re-introduced probing, employing a graduated series of instruments of comparatively large calibre. Weber advocated forcible dilatation, whilst Critchett used laminaria probes.
Though some sort of excision of the sac was practised in antiquity with its cauterization, it was not till Berlin suggested it in 1868 that excision of the sac came into ophthalmology. Two years earlier Laurence had advocated excision of
the lacrimal gland, a procedure first mooted in 1843 by Bernard.
The 19th century was also responsible for the introduction of mydriatics and miotics. Mydriatics have indeed a much longer history, but their widespread clinical application only came with the second half of the century. For pain in the
eyes the Greeks used opium, mandragora and hyoscyamus, a practice strongly condemned by Galen as leading to cataract and other serious complications.

But Galen was not above using hyoscyamus as a cosmetic application for the blue-eyed,
inducing in them a black pupil.Significant, too, is the observation by Pliny that anagallis is used for dilating the pupil before couching operations; this procedure is not mention-ed anywhere else in the old literature, and the reference
is all the more puzzling as anagallis has no mydriatic effect; but in accuracy of details the garrulous Pliny is never too reliable. Whatever vogue mydriatics may have had in Greece and Rome they lost during the succeeding centuries. The
rediscovery came towards the end of the 18th century. Though John Ray, the Father of Natural History in England, recorded in 1686 his observation that a belladonna leaf applied to a small abscess near the eye had caused dilatation of the
pupil, it was not till another century had passed that mydriatics received any attention. This came with the reports of three different observers (Daries, Loder, Reimarus), who independently recorded the mydriatic action of belladonna.
Loder in 1796 and Reimarus in 1797 advocated its use to facilitate cataract extraction, a practice that was adopted in England by Paget of Leicester in 1801 and John Cunningham Saunders in 1809. Himly in particular did much to study
systemically the use and possibilities of mydriatics in ophthalmology, yet it was not till 1831 that atropine was isolated.
The first half of the 19th century was satisfied with general treatment of iritis; the sue of mydriatics for this condition, though indicated as early as 1805 by Schmidt, did not gain any widespread acceptance; von Ammon in 1835 could still
advise against their use in acute cases; and whilst Desmarres in 1847 strongly recommended belladonna in his textbook, his German translator could only report that the drug causes an increase in the inflammation. It was largely through the
advocacy of von Graefe in 1856 that atropine came to occupy its place in modern ophthalmology. No doubt the dispute over the applicability of atropine was in part the consequence of the non-recognition of acute and subacute glaucoma as
distinct from iritis. Even when that recognition came, the deleterious action of atropine in glaucoma was not appreciated; that only came with von Graefe in 1868.
Miotics have a much briefer history. The pharmacology of the calabar bean
was studies at Edinburgh in 1846 and 1855. Fraser, subsequently Professor of Pharmacology at that University, showed its miotic effects in 1862. A year later Argyll Robertson demonstrated its effects on accommodation. In the same year von
Graefe studied its antagonistic action to atropine and employed it to facilitate iridectomy in non-inflammatory glaucoma. It was during the succeeding decade, after von Graefe had shown the danger of atropine in glaucoma, that miotics began
to be employed as therapeutic agents. Eserine was isolated in 1864 and pilocarpine in 1875.
Legend, scholastic disputes, travellers' tales, local patriotism and downright fabrications have all encumbered the quest for knowledge on the early history of glasses. Rock glass must have been known in early times, but even manufactured
glass has a considerable antiquity. A wall painting at Beni Hasan, which accurately depicts the process of glass blowing, is attributed to the period of the XIth dynasty, though there is no evidence of any manufacture of glass in Egypt
till the much later XVIIIth dynasty. References to glass and its manufacture also abound in the Bible. Pliny assigned the origin of glass manufacture to the accidental discovery by Phoenician merchants of a glass-like substance under their
cooking pots, which had been supported by blocks of nitron. It is not unlikely that some such accident - the fusion by heat of impure sodium carbonate with sand, started off the quest for a less brittle and more transparent substance than
was produced in this manner. The manufacture of glass for the production of vases, mirrors and gems of all sorts had developed into an advanced industry long before Roman times.
Legend has it that St. Jerome (c. 340-420 AD) invented
glasses. On more definite evidence the use of glasses in remoter antiquity has been considered. Pliny records the 'Nero princeps gladiatorium pugnas spectabat zmaragdo" and this vague reference to Nero watching gladiatorial contests
with an emerald has been read to mean that he used glasses. The emerald may well have had other uses, as a gem, as the sporting of the green colours of the Emperor, as an amulet - for emeralds had a reputation for strengthening the eye -
and so on. Presumably Nero was short-sighted, but what is known about his sight rather suggests the photophobia of the albino, for which indeed he may have used green glass as a protective. It is certainly a fact that myopia and the weak
sight of old people was well known to the Romans, but nowhere at that period and for many centuries subsequently is there nay reference to glasses. Indeed myopia was regarded as a permanent defect as is shown by the fact that Roman lawyers
considered myopia a vicium perpetuum, diminishing the market value of a slave; and as for presbyopia, the only way Roman patricians knew of overcoming it was by getting a slave to read to them.
Travellers' tales have made China the original centre of glasses. The earliest evidence concerning glasses in China is, however, of considerably later period that the time they made their appearance in Europe. The Chinese probably learnt
about glasses indirectly from Europe through the intermediary of the inhabitants of Malacca.
Magnifying glasses of a sort were known and may have been used in antiquity. The effect of a glass bowl filled with water in showing up details was recognized, as can be seen from a reference in Seneca. Furthermore, Pliny relates that
such bowls were used by physicians for burning. The glass bowl was obviously used as a condensing lens, though it was a wonder to the Romans that cold water should be able to burn. Dimly the biconvex lens was already known.
Alhazen had carried the theory of vision to a sufficiently advanced level almost to have been able to introduce the use of lens. But it was left for subsequent centuries actually to achieve it. The first recognition of these
possibilities seems to have come with Roger Bacon, as seen from a passage not devoid of gross errors. He discusses the use of segments of spheres and shows that letters and small objects on which they are placed appear magnified. "For this
reason such an instrument is useful to old persons and to those with weak sight, for they can see any letter, however small, if magnified enough."
The observation that segments of spheres magnify was not original with Bacon; what constitutes an advance is the clear recognition of their use for old people and those with weak sight. If it was not eye-glasses that Bacon had in mind,
he advocated the loupe or magnifying glass, the forerunner of spectacles.

A painting of Virgil using spectacles:
but glasses were not invented for
at least 1500 years after his death.
References to glasses begin to crowd at the beginning of the 14th century; they, therefore, must have attracted considerable attention towards to the end of the 13th
century. The first medical reference is by Bernard Gordon, Professor of Montpellier (1305). He recommends a collyrium of such potency "that it will enable those whose sight is weak from old age to read without glasses." Guy de Chauliac
(1353) likewise recommends collyria, but adds that when they do not help, recourse should be had to glasses. Incidentally, collyria were time-honoured means for strengthening the sight. Ali ben Isa has laid down explicitly that they who do
not see in the near, "a condition which mainly affects old people" should use styptic medicines; whilst those who see well near by but not in the distance, require medicines which give moist nutrition and bring the moist principle to the
eye.
Attempts to trace the invention of glasses to a particular person have had little success. Fraciscus Redi, a distinguished and learned Professor of Medicine in Pisa, in letters to a friend in 1676, writes that he has a manuscript
dated 1299, in the preface of which a reference is made to the recently invented glasses; " I find myself so oppressed by the years that I no longer have the strength to read or write without the glasses known as spectacles, lately invented
for the comfort of the old souls who have become weak-sighted." Redi further quotes from a sermon (1305) by Fra Giordano da Rivalto: " It is not yet twenty years that the art of making glasses was invented; this enables good sight and is
one of the best as well as the most useful of arts that the world possess." Fra Giordano resided together with Fra Alessandro da Spina in the monastery of S. Catherina at Pisa, and Redi extracted from the manuscript chronicle of the
monastery two references to Spina. One is an obituary notice, Spina having died in 1313, two years after Fra Giordano: "Brother Alexander da Spina, a modest and good man, had the capacity to make things he had seen or of which he had heard.
He made glasses and freely taught the art to others. Glasses had previously been made by someone else who, however, would not say anything about them." Another reference in that chronicle speaks in the same tone and to the same effect,
emphasizing that in contrast to the secretiveness of the original inventor, da Spina freely communicated the secret of the art he had copied.
Thus while Alexander da Spina, a Dominican monk, is generally accepted as the re-inventor of glasses, the original inventor is lost to history. It is in fact doubtful whether there was such as one; it is just as likely that the value of
glasses was found empirically towards the end of the 13th century owing to the accidental use of the somewhat plano-convex glass of some forms of window-plane. Bacon, who had the requisite theoretical knowledge, did not apparently get as
far as glasses, whilst the claims for Salvino Armato of Florence are largely based on the excessive zeal of a Florentine historian, Domenico Manni.
Manni relates that a Florentine antiquary saw a tomb-stone inscription in the now demolished church of St. Maria Maggiore at Florence which read: "Here rests Salvino d'Armato of the Armati of Florence, the inventor of spectacles. God
pardons his sins. A.D. 1317." Manni held that Armato was the secretive inventor spoken of in the references to da Spina, and this flimsy view has somehow gained widespread acceptance.
What looked like more conclusive evidence was published in 1845 by Casemaecker of Ghent. A rather lurid story is told of Roger Bacon - incidentally translated into a Belgian - fleeing before Papal wrath and passing on his invention of
spectacles to a friend, from whom it was that da Spina heard of glasses. Bacon himself was most anxious not to attract further attention from the Church, as he was already in heavy disfavour for his other works. To Hirschberg, this tale,
along with its other lurid details, sounded like a bad detective story, and on investigating it he found that though it had been accepted as authentic history it was nothing more than pure invention written by a journalist for its reputed
author, an optician.
It was therefore somewhere towards the 13th century that glasses came to be introduced. Glasses began to have a vogue towards the middle of the 14th century; and painters and sculptors could not resist the temptation to endow biblical
figures with these accessories. Glasses were even deemed necessary in the Garden of Eden. Public documents make references to them and wills dispose carefully of spectacles, for they were still a costly item. It was not till the beginning
of the 16th century that the concave glass began to be used; Pope Leo X, painted by Raphael between 1517 and 1519, is depicted holding a concave lens, and a number of later references in books abound. But it was not till Kepler (1604) that
the whole subject was clearly conceived.
Spectacles were not well received by the oculists. Bartisch scornfully dismisses them; he could not conceive how an eye that does not see well would see better with something in front of it. Even after Kepler, collyria for weak sight
prospered. Nevertheless a great deal of practical and useful information was being collected by humbler vendors of glasses, and this was well systematized in an utterly unscientific treatise published in Spain in 1623 by Daza de Valdés,
"licentiate and notary of the Inquisition in the City of Seville." The use of high convex lenses after cataract operations is clearly indicated, whilst a scale of different strengths of reading glasses for different ages is laid down. For a
man between 30 and 40, lenses of 2 degrees were needed; for one aged between 70 and for higher ages lenses of five to six degrees. Women required more than double the strength, for not only do they perform more delicate work, but their eyes
are naturally weaker.
Almost down to the middle of the 19th century the fitting of glasses was the prerogative of untrained vendors — mostly itinerant, who combined this business with the other occupations usual to pedlars. Oculists took but the slightest
interest in the matter, at the most recommending a patient to go to a shop and select the most suitable pair obtainable. The range of choice was of course not wide. The stock in trade consisted of glasses after cataract operation, glasses
for old sight, glasses for short sight and occasionally glasses for "old sight of young people". Astigmatism was not known till Young demonstrated it in his own eyes in 1801; that a correction was possible was not realized till Airy
designed a suitable cylindrical lens in 1827. But even so it was not till after Donders and the subsequent introduction of retinoscopy that the treatment of astigmatism assumed any tangible practical form.
Indeed, almost until Donders glasses met with a remarkable hostility. During the earlier part of the 19th century there was much hostility, largely the result of Beer's attitude to them, for Beer had little more use for them than
Bartisch. Weller, in a standard book in 1832, advises against concave lenses if the eye is to be saved from deformation, and is to preserve its ability to become far-sighted after the age of 40. Sichel, another important contemporary writer,
sees in concave lenses the cause of old sight, whilst yet another author blames glasses for the development of short sight. Here and there, particularly in England, an isolated voice was raised pleading for the use of glasses. In this
connection the charlatan Rowley deserves to be remembered, as also Kitchiner and Lawrence. The trial case was first introduced in 1843, and in the same year Küchler introduced test types for near. Eleven years later Jaeger introduced test
types for both near and distance, though it was left to Snellen to put these on a scientific basis. By the use of the ophthalmoscope Jaeger paved the way for the objective determination of refractive errors, in the development of which the
names of Bowman (1859) and Cuignet (1875) stand out. But it was largely the work of Donders that made the problems of refraction and the rational use of glasses part of the ophthalmic creed.
The introduction of prisms into ophthalmology also dates from this period. First introduced by Kepler, pioneer work in their clinical application had been carried out by Wells in 1792; yet it was not till Donders in 1847 and especially
von Graefe in 1857 showed their value in muscle insufficiency, that any serious attention was given to their possibilities.

In this later life, Benjamin Franklin developed presbyopia. As he was also myopic,
he got tired of constantly having to interchange two pairs of glasses. So he decided
to figure out a way to make his glasses let him see both near and far. He had two pairs
of spectacles cut in half and put half of each lens in a single frame to make a bifocal.
The evolution of the spectacle frame has a history of its own. The oldest spectacles, known to us from a painting by
di Modena in 1352, consisted of two lenses in rims, joined centrally. The inconvenience of holding such glasses in
position for any length of time led to a modification suggesting sugar-tongs. Metal rims gave way to leather ones; such a pair has been found preserved within a book. An early modification — incidentally recommended by Savodarola — was to
secure the glasses by a tape tucked under the hat, a method rather reminiscent of the Chinese way of binding the glasses to the head gear. Various forms of lorgnette followed. The original attempts at ear-rails added greatly to the already
heavy weight of spectacles. It was only towards the end of the 18th century that passable ear-rails came to be introduced. These were followed by glasses with nose-pieces having a spring, a marked advance on the much earlier nose-riders
which were kept in position by the pressure the rims exercised on the nose. Gold, silver, steel, fish-bone, horn, wood and leather have all been used for the making of the spectacle frame.

From the moment of their invention, people had problems in deciding on how to keep glasses on. The present frame with sidepieces resting on the were invented by Edward Scarlett in 1730.
While the problems of wearing glasses nowadays present little problems, some poor souls are less certain about the correct way of wearing a monocle as shown by the following article found in Sunday Times Magazine, 1999:
Dear Mrs. Mills,
I have worn a monocle on and off for the past few years. I now feel totally comfortable and indeed confident with it. However, I am anxious to know the correct etiquette, if any, that goes with the wearing of an eyepiece. I do
entertain on a regular basis — luncheons, dinners and so on — and I'm desperate to ascertain the correct procedures when receiving dignitaries and, of course, female company.
DPC, Lincs
Dear DPC,
While the monocle should be worn whenever needed for seeing clearly (ie, reading, shooting, neurosurgery), it is also your responsibility to maintain its silly-ass yet, paradoxically, rakish image. So, for instance, it should be worn when eating soup so that you can exclaim "Gosh" (or "Crikey" in extreme duress), put on a surprised expression and allow the monocle to fall into the bowl
— a minor coup de théâtre that will give you the moral high ground. On the other hand, when being introduced to a lady wearing a low-cut dress, never fail to screw the monocle tightly into your eye socket and draw! "Hellloooo" while examining her cleavage closely. Extra kudos is obtained by sounding like Terry-Thomas.
Mrs. Mills
Why the pupil is black was a problem that attracted the attention of Roman writers, but the explanations they gave are merely of historical interest. It was held that the moisture in the eye was black; it was also suggested that
the blackness resulted from the eye being a sort of deep trough. Yet the Ancients were also acquainted with the fact that some animal eyes are lustrous. Pliny observed that the eyes of nocturnal animals, such as cats, are brilliant in the
darkness. The explanation had to wait for many centuries. Mariotte made some approach to it when he noted that the reason a dog's eye is luminous was that its "choroid" is white, and that hence the image of a light is painted on it clearly,
whereas in man and in animals with black "choroid" no such clear image could be formed. This is a dim realization of the existence of the tapetum. Bidloo in the 17th century appreciated that no animal eye radiates light that it had not
received, but it was not till 1810 that the simple observation that animal luminosity disappears in complete darkness was established by Prevost. This laid forever such views as those that regarded animal luminosity as a sort of
phosphorescence; or that the radiation by night came from light absorbed during the day, or yet again that luminosity was the result of some such internal activity as is seen in the firefly. "Naked electricity" was yet another explanation
that had passed muster. All these views had been invoked to explain the supposition that animals with lustrous eyes could see in the dark.
Further advance towards a clearer understanding was supplied by the work of
Rudolphi in 1821. He showed that the luminosity of an animal eye depended largely upon the direction of the ingoing rays. That furthermore the problem was a purely physical one he showed by the observation that the eye of a decapitated cat
was just as effective for the production of luminosity as that of the living animal. A few years later Esser went further still by showing that the decapitated cat was really the better as the pupil was widely dilated.
That, at least partially, an optical problem underlay this animal luminosity was indeed also realized, more that a century earlier, when Mery in 1703 found that the luminosity of the cat's eye could easily be viewed when the
animal was held under water. He appreciated that it was more than mere dilatation of the pupil consequent on suspended animation that was responsible for this phenomenon, and his explanation was that the water filled in unevenness of the
cornea. The correct explanation was advanced by de la Hire six years later, when he argued that the cat's fundus was seen owing to abolition of corneal refraction under water; that consequently the rays emerged divergent, and some of them
were thus caught by the observer's eye.
These considerations all seemed to have no practical significance. Even when luminosity in human eyes was observed the problem still remained an academic exercise. Duddell, in 1735, had noted the spontaneous luminosity of the
eye of the human albino, as Woolhouse before him had observed it in white rats. Later in the century Fermin had noted luminosity of the eye of an Ethiopian albino (and incidentally held that this patient could thus see at night, because his
eyes were like those of night animals). Further interest in spontaneous luminosity of man was aroused by Richter's observation (1790) that in one form of blindness luminosity was present. This led Beer to introduce the term amaurotic
pseudo-glioma. Spontaneous luminosity was also noted in aniridia in 1829 by Beer.
No attempt to explain this spontaneous luminosity in man was made, though a close approach had been made to the explanation in the case of animals. The observation of Purkinje in 1823 that under certain conditions of
illumination human eyes could be made luminous, passed unnoted. It had to be rediscovered independently by Cumming in 1846 and by Brucke in 1847. It was finally realized that the observer had to stand in the path of the emerging rays.
Brucke indeed came near to inventing the ophthalmoscope when he looked through a tube placed in the flame of a candle illuminating the eye, and thus caught some of the emergent rays.
A conscious attempt to see the fundus was made by Kussmaul at about the same time (1845). On the basis of de la Hire's explanation of Mery's observation of the fundus of a cat submerged under water, he applied to the eye a
plano-concave lens of the same power as the cornea, hoping to be thus enabled to see the optic nerve in the living human eye — a procedure that " should be of great value in the diagnosis of certain eye diseases". He failed, for he did not
realize the necessity for illuminating the eye. Babbage, of calculating machines fame, is another precursor; but whether he acted just as consciously as Kussmaul and what exactly he invented, is not definitely known. There is no documentary
evidence as to what he made and what he showed to Wharton Jones in 1847, except the latter's account seven years later.
By this time the optical problem underlying luminosity of animal eyes and of the human eye under certain conditions had nearly reaches its solution. Indeed, the fact that the eye was not luminous under normal conditions
because it forms an optical apparatus which returns entering rays to a focus at the source of illumination, had been indicated by the rather crude experiments of Kussmaul. Though he had failed to view the fundus in the living eye by
neutralizing the refraction of the cornea, he showed that by further deranging the optical structure of the eye through removal of both the cornea and lens the fundus could be seen, and that it could likewise be seen if some vitreous was
extracted and the retina came forward.
The crowning achievement came when Helmholtz announced the invention of an "eye-mirror" in December, 1850. His ophthalmoscope consisted not of a mirror but of plates of glass, four plates being used to increase the number of rays
reflected into the eye. The illumination was of necessity poor. Modifications followed each other in rapid succession, the silvered mirror with a central hole arriving within a year. Two great improvements were likewise introduced at an
early stage. Helmholtz's original ophthalmoscope was mounted with a holder for one lens, and lenses had to be changed constantly for eyes of different refraction. Rekoss, a technician, introduced a revolving disc carrying a series of lenses,
whilst Ruete in 1852 introduced the indirect method of ophthalmoscopy. Thereafter an endless series of modification and improvements followed. The refracting ophthalmoscope was introduced at about 1870, whilst tentative electric
ophthalmoscopes were brought out about fifteen years later, one of the earliest being that of Juler in 1886. Search for the ideal source of illumination led to attempts with oil, petrol, gas, daylight and almost every conceivable
monochromatic flame.

Early indirect ophthalmoscope. Note the inverted image is
illuminated with the light from a lamp placed on the table.
The introduction of the ophthalmoscope in clinical ophthalmology was facilitated through it is brilliant application by von Graefe and his
colleagues. Enthusiastically received by them it did not fare so well elsewhere. It was argued that it is dangerous for a diseased eye to be submitted to the strain of all this illumination. Some, more patronizingly, held that it might be
quite a useful instrument for such oculists as have poor sight. Dixon of London, 1853, expressed the fear that its use might lead to amaurosis. In France, qualified support was given to the ophthalmoscope — as indeed was the case with
earlier models having a concave lens only. It was Anagnostakis who, in 1854, popularized the instrument in France by a series of excellent observations. In England, pioneer work was done by Spencer Watson, and ardent support came from
Bowman, though as late as 1855 the Lancet could still speak sceptically of its value. In other countries, Holland excepted, it penetrated even more slowly. Yet by the time the First International Ophthalmological Conference was held
in 1857 the ophthalmoscope had come to be sufficiently significant to claim the first discussion.

Ophthalmoscopes from the 19th century.
Within a decade the ophthalmoscope had revolutionized ophthalmology. For one thing, it forced attention to the refractive state of the eye, supplying at the
same time objective means of determining it. In no small measure the work of Donders is the result of the introduction of the ophthalmoscope. But even more far-reaching was the demolition of the age-long puzzle of amaurosis. At one stroke
endless guesses, speculations, theories and discussions became meaningless. A new conception of glaucoma emerged early, even if at first it was held that in glaucoma no changes were present in the fundus, a view that was replaced by the
belief that swelling of the disc was present, But by 1855 von Graefe, who with others had fallen into the earlier error as to swelling, demonstrated excavation and retinal pulsation - and iridectomy as a method of treatment of the hitherto
hopeless and badly understood disease followed rapidly. A new chapter — medical ophthalmology — was opened by von Graefe in 1855 and Heymann in 1856 by the description of renal retinitis, whilst in 1860 von Graefe presented a boon to
neurology by his observation of bilateral papilloedema. Coccius in 1853 described detachment of the retina and indicated retinitis pigmentosa. Thrombosis of the central vein was recognized by Liebriech in 1855, whilst von Graefe recognized
embolism of the central artery in 1860.
 ... ...
Early illustrations of the fundi from the 19th century when
ophthalmoscopes were first invented. The picture on the left
shows advanced glaucoma and on the right retinitis pigmentosa.
Amaurosis, the condition which had been defined as one in which the patient saw nothing and the oculist also saw nothing , had ceased to exist.
Roman seals for the preparation of collyria constitute the earliest records of ophthalmology in England. A number of these have been unearthed and one, found in
Ireland, presents an interesting historical problem, for the Roman invasion is
not supposed to have included that country. These seals are not different from those found elsewhere, so that if any native ophthalmology existed, it does not appear to have influenced the imported practice. Some evidence of ocular
treatment in Saxon times is furnished by the extant Saxon Leechdoms; the records speak of a number of herbs, amongst which, as James points out, eyebright is absent — an interesting omission, for eyebright figured large in later herbals.
Much more significant than this primitive ophthalmology are the learning and investigations that were to be found in the monasteries of Norman England. It is more than likely that Roger Bacon's contributions represent not an isolated
brilliant achievement, but the acme of less far-reaching work that was going on steadily in these secluded seats of learning. James draws attention to Robert Grosseteste, Bacon's teacher, whilst the work of John de Peckham has passed into
history — his is the first discussion on the refraction of concave lenses.
The 14th century supplies the first native ocular treatise; Sir D'Arcy Power speaks of it as one of the lesser writings of John of Arderne. There are available
the original Latin text and an early English translation; a full abstract of it has been published by James in his "History of Ophthalmology in England." It is largely a formulary and its most interesting passage is an autobiographical
reference. It is only towards the end of the 16th century that an ophthalmic literature worthy of the name makes its appearance in England.
Short chapters on the eye occur in Philip Barrough's Method of Physick, the first edition of which appeared in 1583. They are are of no particular significance. Of not much greater significance is Walter Bayley's Briefe
Treatise touching the Preservation of the Eyesight, consisting partly in Good Order of Diet and partly in Use of Medicine, first published in 1586. Bayley was physician to Queen Elizabeth, but his knowledge of ophthalmology extended to
little beyond doubting the efficacy of urine for bathing the eye and recommending ale as strengthening the sight. Somewhere between 1586 and 1589 appeared a translation of Jacques Guillemeau's Maladies de l'Oeuil, a useful
summary of the existing knowledge, mainly on Greek and Arabian sources, by a pupil of Ambroise Paré. The century closed with another translation, Andreas Laurentius' Discourse of the Preservation of the Eyesight. In the second decade
of the 17th century appeared another tract, Two Treatises concerning the Preservation of Eyesight, the first one being a reprint of Bailey's essay, whilst the second - an anonymous "scissors and paste" production drawn from the
writings of Benevenutus of Jerusalem, Riolanus and Fernelius — contains nothing new. British ophthalmology had yet to be born.
Its beginnings were created by Richard Banister in 1622. In that year he reissued the translation of Guillemeau's book, for this "worke ... being long since out of print, it is not now to be bought for money." He
sent it "abroade again, that those which delight to labour in this Art, may runne the readier way to the better successe." He added a Breviary, "something of mine owne, that through my experience they may finde
at first, what I was learning long." The something of his own is not always useful, but contains much bears the stamp fo the experienced oculist. Much the most significant passage is the one in which hardness of the eye is described as a
diagnostic and prognostic feature in the treatment of gutta serena — an observation that fell on stony soil and had to be rediscovered in the 19th century. Banister's Breviary is also of inestimable value as a document on the
social standing of oculists in that age. He relates in a delighfully naïve way how he came to devote himself to the study of diseases of the eye; and in criticizing ignorant practitioners he has left a sidelight on the practice of
ophthalmology in his days: —
"...My special breeding has beene in the general skill of Chirurgeries. ... I left the greatest masse of that unmeasurable mysterie, as a heape too heavy for my undergoing; to take up onely some particular pieces, wherein
I might the better proceed to some perfection: choosing rather to walk in a right line, whose very beginning points to a certaine end; then to run in a ring, whose mazefull compasse foretells much paine with little progresse, or a long
journey without an Inne. ....I thought the Art would be no loser by me, if I did let goe many parts of her, to hold the rest more sure and certaine. And finding some defects in mine owne eyes, I chose their cure for my care, that so I might
benefit my selfe first, and otheres after by mine owne experience: unto this also I adioyned the helpe of Hearing by the instrument, the cure of the Hare-lip, and the wry Necke. When in the threshold of my practice, I could couch the
Cataract, and so began to gaine some name of an Oculist, I laboured to advance my skill by the advice of the most skillfull in those times: ...Byt in observing them, I noted much practice, but little Theories; therefore not contenting my
selfe to have but one string to my bow, lest a time of night might overtake me wanting oyle in my lampe; and labouring to bee as cunning in knowledge of the reason, as perfect in practice upon the occasion; I addressed my selfe to the study
of divers best approved Authors, ... And hereby wee see the boundlesse boldnesse of many women, who for lacke of learning, cannot be acquainted with the Teoricke part, and yet dare venture on the Practicke. I beleeve, scarce three of
thirteen hundred, can define or describe the names and natures of the hundred and thirteene diseases of the eye; to shew whether they be in the Humors, Membranes, Muscles, Optick Spirits, etc., yet having snatched up some one or two
medicines onely, they thinke themselves armed against all diseases ... Let these women therefore either applie themselves to learne the grounds of their practice, or leave their practice to them that are better grounded; that so they may
cease by their ignorance to make them blinde, that by our Arte might be made to see. Many have come from these to me, lighted more by sorrow than by sight, with their eyes full of teares, but empty of opticke humors. And yet these
firebrands that choke and smoke folks eyes out, can take hennes, chickens, and such reasonable rewards for their unreasonable wrongs."
Further on he relates: "Of proud quacksalving Mountebankes, that would undertake all Cure, and performe few."
"Such are they, that promise to make blind people see, deafe people heare, and to cure the Stone and Rupture by cutting. In the methodicall practice and cure of blind people, by couching of Cataracts, our English Oculists
have alwayes have an expeciall care, according to Arts, to couch them within doores, out of the open aire, to prevent further danger. Yet some of these Mountebanks take their patients into open markets, and therefore vaineglories sake, make
them see, hurting the Patient, only to make the people wonder at their rare skill. Some other make Scaffolds, on purpose to execute their skill upon, as the Frenchmen, and Irish man did in the Strand, making a trumpet to be blowne, before
they went about their work. But these were not long suffered to use these lewd courses, before they were called before the company of the Chirurgions: being sharply reprooved, soone left the City, and their abusive practice. ...Beside this
lewd practice, some of the afore mentioned, will cut for the Stone and Rupture, when by other meanes they might performe the Cure and wicked practice.... The skins of which, these Empericks take away, they stuffe with wooll, or flax, to
make them shew the greater, and these they hang upon a wall, or post, in the open markets, to make their gelding skill more knowne."
Banister was an itinerant oculist. He relates of his cures in Norwich, London, Lincoln and elsewhere, cures testified by the magistrates. His apologia for his itinerant activities and advertisements is delightful: —
"...It maybe, some will object, as they have done, I need not have travelled so farre form home to do these Cures: for they would have come to me. I answere, Three causes made me to do this: first, when I was abroad and
made my selfe knowne in a strange place, I did see more defected Eyes in one moneth, then I should have seen in halfe a yeare at my owne house, whereby my knowledge and skill was increased so much the more, for the true judgement in
defective Eyes. Secondly, if I had not made my Practice publikely knowne abroad, I should have had no resort to me at home, so that my small talent might have been hid in oblivion. Thirdly, Many poore people that wanted help, as well as
rich, were not able to travell so far to me for helpe; both in respect of the weakness of their bodies, and disability of their estates, which I willingly helped as wel as others."
An important document on that period is published by James. It consists of an anonymous manuscript in the British Museum, and James is inclined to regard it as possibly the work of a son of Richard Banister, though some claim could be
made for Richard Banister himself. In a "Briefe discourse of ye Chefeste Oculistes" there is much light thrown on the ophthalmic practice of the day.
There was Luke of Erithe,
" a man that lived in greate fame and credite had the greatest practise and sumes of money for he hathe had from XX to LX L for Cataracke couchinge ... He neuer set upe bils that I heard of but those that desyred his
helpe and dwelled far from him he would apponynte a tyme to come to them and would wyshe ym to gyve notis of his comminge to alle they knewe stoode in need of his helpe."
No less interesting was Mr. Surphelete, a man,
"of axeolente Dyet and crusty fasion of bodye. He lived till he was fouere score yeares of age lived moste in Norfolke & dyed at Linn and in good estate. He lay 2 or 3 years at a barber's house at Linn to whom he taught
som skille, who nowe professethe it with weak Understandinge and gyven to drinke I cannot com'end this Mr. Surphlete for any extraordinarye skille though of longe experience."
But most interesting of all was Henry Blackbourne,
"who travelled contynuouslye from one market towne to another, who could couche ye Cataracke welle, cure yt, Laye oa scar Lipe, set a crockt necke strayght & helpe deafness. Though he could doe good in these cures yet he
was soe wickedlye gyven that he would cousen & deceave men of great som of moneys by taken incurable diseases in hand. He was lust amorously gyven to seueral women so that his coseninge made him fearfully to flee from place to place and
often changed his name and habits in divers places & was often imprisoned for women. His skille was excelente, but his vices ... longus, his practeste was this, yf he made a blinde man see; after he had couched ye Cataracke ...yf he
herde they welle he woulde see ym agayne, yf not he would neuer come at ym. If cum payne or accedentyles fell out they receaved no comforte from him....Though before I com'ended him for a good oculist it was for his manuel operation & not
his method or medicines. He hyed in Kent after he had thoroughly travelled alle partes of the lande, he left no memorie of his gaynes or gettinges his wicked lyfe was suche that I thinke he had not one friend that he trusted, but alwayes
that he got he caryed about with him. He was often deceaued of great sums of money yet neuer robbed. He hyed but in meane estate had one sonne and left him nothing."
When the curtain is thus first lifted on English ophthalmology, there is not much to excite admiration. And the rest of the 17th century offers little relief. Robert Turner in 1654 and again in 1665 brought out " The Compleat Bone Setter,
" in which a section is devoted to the Perfect Oculist, this itself being nothing more than an unacknowledged adaptation of the anonymous tract published in 1616. But the century did not close altogether in this bleak fashion.
Apparently the orthodox practitioners were turning to the study of the eye. Daubigney Tuberville of Salisbury was a properly qualified practitioner and belonged to an old family. He had a great reputation and his services were widely sought;
thought not on good terms with the Court physicians he was called in to treat the future Queen Anne. The Philosophical Transactions contain two letters of his, in one of which an account is given of the use of a magnet to withdraw a
piece of steel embedded in the "iris" [limbus]. William Briggs' Latin treatise on the anatomy of the eye, containing the first account of the optic disc, belongs to this period. Briggs was more than anatomist; his "Theory of Vision" is of
interest as showing the searching that was going on for new explanations. Another qualified practitioner of that period, though hardly worthy of consideration together with Turberville and Briggs, is William Coward. His Latin
Ophthlamiatria, published in 1706, is of little significance.
Coward's book was one of three that appeared in the first decade of the 18th century. The two others were even more insignificant than his. A brief Treatise of the Eyes by William Crosse is a rather long advertisement of the
author's secret remedies, whilst Sir William Read's Treatise for the Eyes is an unacknowledged reprint of Banister's Breviary and the translation from Guillemeau, together with a rodomontade on Read's manual dexterity and
styptic water. Read's Short but Exact Account of all the Diseases Incident to the Eyes is but the same production with a different title page; it is not even a reprint. A rather more significant publication was Peter Kennedy's
Ophthalmographia, published in 1713; if unoriginal, it is at any rate honest.

Quack flourish in all ages, and the eye has always been a happy hunting ground for such practitioners.
No one
will question the statement that the 18th century was the heyday of ophthalmic quackery. Sir William Read (the inserted picture shows his advertisement), who was knighted by Queen Anne, set the fashion in high places, and was followed
by Roger Grant and the whole tribe of the Chevalier Taylor.
Sir William Read flourished from about 1675 till his death in 1715; he was succeeded by Roger Grant; each of these men was illiterate. Read was the son of a Suffolk
cobbler and apparently could not even sign his name, while Roger Grant rested his pretensions to practise ophthalmology on the fact that he had lost an eye in the Emperor's service in the continental wars; thus reversing the case of the
gladiator alluded to by Martial:
Oplomachus nunc es, fueras ophthlamicus ante fescisti medicus quod facis oplomachus.
The conflict between orthodoxy and quackery was to last for the rest of the century, largely because of the indifference of the profession to ophthalmic matters. Benedict Duddell had to complain in 1729 that surgeons undertook
treatment of eye conditions without the necessary knowledge: "to the question how a certain surgeon did to know the different natures of the distempers of the eye: His answer was that he undertook all. If his operation succeeded, so much
the better; if not the patients could but be blind, or in danger of being so, as they were before." In such an atmosphere charlatanism could not but prosper, especially as the charlatan was often well grounded in the subject; Woolhouse and
the Chevalier Taylor were certainly the equals in knowledge to most of the more orthodox oculists. Though Cheselden, who introduced the operation for artificial pupil, and Duddell, who wrote an excellent monograph on the cornea, flourished
in the first half of the century, significant names of surgeons who were interested in eye diseases begin to appear only in the second half. Amongst the earliest was Sharp of Guy's Hospital, a pupil of Cheselden; he contributed the single
incision by puncture and counterpuncture to the operation for extraction of cataract, whilst towards the end of the century Ware contributed very largely to the recognition of the venereal origin of neonatal ophthalmia. Yet even so,
Benjamin Bell, writing in 1785, had to complain that the difficulty in deciding whether couching or extraction is the better operation, is due to the fact that operations are left to itinerant practitioners.
The century closed as it began — by plagiarism. William Rowley's Treatise of One Hundred and Eighteen Principal Disease of the Eyes is an unacknowledged and faulty translation of Plenck's Doctrina de Morbis Oculorum.
Quackery, charlatanism and plagiarism is the unenviable record of the 18th century in England, a century during which modern clinical ophthalmology was being built up by orthodox practitioners in France. But the growing number of surgeons
who studied eye disease and the advent of Porterfield in Edinburgh and Thomas Young in London, carried the promise which matured early in the succeeding century.
The founding of "Moorfields" was its first fruit. Started by John Cunningham Saunders in 1805 as an Eye and Ear Infirmary, it became transformed two years later into an exclusively ophthalmic hospital, the first of its kind in the world.
From Moorfields emanated a new conception of the place of ophthalmology in medical practice; when the need for orthodox practitioners with knowledge of eye disease was satisfied, quackery as a force vanished without a struggle. After the
foundation of Moorfields ophthalmology in England went from strength to strength. Other hospitals followed in rapid succession — the West of England Eye Infirmary at Exeter in 1808, and institutions at Bristol and Manchester in 1810 and
1814. The second hospital to be established in London was the Royal Westminster Ophthalmic Hospital founded by George James Guthrie in 1816. At this hospital in 1817 the first course of lectures on disease of the eye was established. The
Central London Ophthalmic Hospital came in 1843, the Western Ophthalmic Hospital in 1856, the Royal Eye Hospital was established a year later. The movement for eye hospitals stimulated the opening of ophthalmic departments in the general
hospitals. Many more years were, however, to elapse before it came to be generally accepted that ophthalmology required an undivided allegiance; not a few of the great ophthalmologists of the 19th century were general surgeons as well as
ophthalmologists.
The activities of the new generation of ophthalmic surgeons led to the publication of a number of text-books, and in the third decade three books — the first adequate books on ophthalmology in English — made an almost simultaneous
appearance: William Mackenzie's in 1830, Sir William Lawrence's in 1833 and Richard Middlemore's in 1835. These, like Wardrop's Essays on the Morbid Anatomy of the Human Eye, were no longer acknowledge or unacknowledged translations of
continental books, but represented contributions to ophthalmic literature. Henceforth on the exchange of world ophthalmology had come to barter not to borrow.
The earliest effort for an ophthalmic journal came with the publication by John Richard Farre of a Journal of Morbid Anatomy, Ophthalmic Medicine and Pharmacological Analysis, with Medico-Botanical Transactions communicated by
the Medico-Botanical Society. Only one issue appeared, and in a way the journal may be considered as the precursor of the Royal London Ophthalmic Hospital Reports, first published in 1857. In the meantime Richard Middlemore in
1837 had mooted the idea of a Journal of Ophthalmology, but nothing beyond a prospectus appeared. The first exclusively ophthalmic journal, planned on a wider scale than the Ophthalmic Hospital Reports, came in 1864 with the
publication of the Ophthalmic Review, edited by John Zachariah Laurence and Thomas Windsor. The journal, a quarterly, lasted barely four year. The second Ophthalmic Review began to appear in 1881, and british ophthalmology had
yet to see the rise of the Ophthalmoscope (1903) before it achieved its present central organ in The British Journal of Ophthalmology (1917).
The names of many of the makers of 19th century ophthalmology in the British Isles — Bowman, Laurence, Hutchinson (1828-1913), Tay, Argyll Robertson, Nettleship (1845-1913),
Doyne, Marcus Gunn (1850-1909), Coats (1876-1915) to mention only a few — have become household words in ophthalmic practice. And there is reason to believe that they have left to
their successors not only a record but an inspiration and a tradition.
ϟ
Fonte do texto e imagens:
MRCophth
2.Jan.2011
Publicado por
MJA
|